Simultaneous subcutaneous implantable cardioverter-defibrillator and leadless pacemaker implantation for patients at high risk of infection: a retrospective case series report.
{"title":"Simultaneous subcutaneous implantable cardioverter-defibrillator and leadless pacemaker implantation for patients at high risk of infection: a retrospective case series report.","authors":"Giuseppe M Calvagna, Sergio Valsecchi","doi":"10.1007/s10840-023-01684-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The subcutaneous implantable cardioverter defibrillator (S-ICD) and leadless pacemaker (LP) are alternative options for patients at high risk of infection requiring ICD and pacing therapy. In this analysis, we described the simultaneous implantation of S-ICD and LP in patients with high infectious risk.</p><p><strong>Methods: </strong>The study cohort comprised patients referred to our institution for ICD implantation due to high-risk factors of infection.</p><p><strong>Results: </strong>Between 2018 and 2022, 13 patients were referred, including 11 with infected ICD and 2 for first ICD implantation in the presence of high-risk factors. In cases of infected ICD, successful extraction was performed using a mechanical dilatation technique. Reimplantation was delayed until resolution of infection with antibiotic therapy. The devices were implanted during a single procedure, with S-ICD implantation following LP placement for verification of sensing adequacy through surface ECG screening. Suitable vectors for sensing during inhibited and ventricular pacing were identified in all patients. Defibrillation testing was effective, and no issues with double counting or undersensing were observed. The postoperative period was uneventful, and during a median follow-up of 35 months, no complications or infections were reported. The median ventricular pacing percentage was 5%, and a single inappropriate shock episode due to myopotential interference was reported and resolved by reprogramming the sensing vector.</p><p><strong>Conclusion: </strong>Simultaneous implantation of S-ICD and LP is feasible and safe in patients at high risk of infection requiring both ICD and pacing therapy. This combined approach provides an effective solution for these patients.</p>","PeriodicalId":16202,"journal":{"name":"Journal of Interventional Cardiac Electrophysiology","volume":" ","pages":"943-951"},"PeriodicalIF":2.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Interventional Cardiac Electrophysiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10840-023-01684-9","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/8 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The subcutaneous implantable cardioverter defibrillator (S-ICD) and leadless pacemaker (LP) are alternative options for patients at high risk of infection requiring ICD and pacing therapy. In this analysis, we described the simultaneous implantation of S-ICD and LP in patients with high infectious risk.
Methods: The study cohort comprised patients referred to our institution for ICD implantation due to high-risk factors of infection.
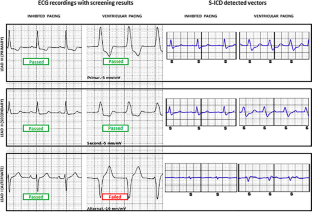
Results: Between 2018 and 2022, 13 patients were referred, including 11 with infected ICD and 2 for first ICD implantation in the presence of high-risk factors. In cases of infected ICD, successful extraction was performed using a mechanical dilatation technique. Reimplantation was delayed until resolution of infection with antibiotic therapy. The devices were implanted during a single procedure, with S-ICD implantation following LP placement for verification of sensing adequacy through surface ECG screening. Suitable vectors for sensing during inhibited and ventricular pacing were identified in all patients. Defibrillation testing was effective, and no issues with double counting or undersensing were observed. The postoperative period was uneventful, and during a median follow-up of 35 months, no complications or infections were reported. The median ventricular pacing percentage was 5%, and a single inappropriate shock episode due to myopotential interference was reported and resolved by reprogramming the sensing vector.
Conclusion: Simultaneous implantation of S-ICD and LP is feasible and safe in patients at high risk of infection requiring both ICD and pacing therapy. This combined approach provides an effective solution for these patients.
期刊介绍:
The Journal of Interventional Cardiac Electrophysiology is an international publication devoted to fostering research in and development of interventional techniques and therapies for the management of cardiac arrhythmias. It is designed primarily to present original research studies and scholarly scientific reviews of basic and applied science and clinical research in this field. The Journal will adopt a multidisciplinary approach to link physical, experimental, and clinical sciences as applied to the development of and practice in interventional electrophysiology. The Journal will examine techniques ranging from molecular, chemical and pharmacologic therapies to device and ablation technology. Accordingly, original research in clinical, epidemiologic and basic science arenas will be considered for publication. Applied engineering or physical science studies pertaining to interventional electrophysiology will be encouraged. The Journal is committed to providing comprehensive and detailed treatment of major interventional therapies and innovative techniques in a structured and clinically relevant manner. It is directed at clinical practitioners and investigators in the rapidly growing field of interventional electrophysiology. The editorial staff and board reflect this bias and include noted international experts in this area with a wealth of expertise in basic and clinical investigation. Peer review of all submissions, conflict of interest guidelines and periodic editorial board review of all Journal policies have been established.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


