Michalina A Montaño, Takudzwa Mtisi, Ntokozo Ndlovu, Margaret Borok, Agatha Bula, Maureen Joffe, Rachel Bender Ignacio, Maganizo B Chagomerana
{"title":"Characterizing HIV status documentation among cancer patients at regional cancer centers in Malawi, Zimbabwe, and South Africa.","authors":"Michalina A Montaño, Takudzwa Mtisi, Ntokozo Ndlovu, Margaret Borok, Agatha Bula, Maureen Joffe, Rachel Bender Ignacio, Maganizo B Chagomerana","doi":"10.1186/s13027-023-00548-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In East and Southern Africa, people with HIV (PWH) experience worse cancer-related outcomes and are at higher risk of developing certain cancers. Siloed care delivery pathways pose a substantial barrier to co-management of HIV and cancer care delivery.</p><p><strong>Methods: </strong>We conducted cross-sectional studies of adult cancer patients at public radiotherapy and oncology units in Malawi (Kamuzu Central Hospital), Zimbabwe (Parirenyatwa Group of Hospitals), and South Africa (Charlotte Maxeke Hospital) between 2018 and 2019. We abstracted cancer- and HIV-related data from new cancer patient records and used Poisson regression with robust variance to identify patient characteristics associated with HIV documentation.</p><p><strong>Results: </strong>We included 1,648 records from Malawi (median age 46 years), 1,044 records from South Africa (median age 55 years), and 1,135 records from Zimbabwe (median age 52 years). Records from all three sites were predominately from female patients; the most common cancers were cervical (Malawi [29%] and Zimbabwe [43%]) and breast (South Africa [87%]). HIV status was documented in 22% of cancer records from Malawi, 92% from South Africa, and 86% from Zimbabwe. Patients with infection-related cancers were more likely to have HIV status documented in Malawi (adjusted prevalence ratio [aPR]: 1.92, 95% confidence interval [CI]: 1.56-2.38) and Zimbabwe (aPR: 1.16, 95%CI: 1.10-1.22). Patients aged ≥ 60 years were less likely to have HIV status documented (Malawi: aPR: 0.66, 95% CI: 0.50-0.87; Zimbabwe: aPR: 0.76, 95%CI: 0.72-0.81) than patients under age 40 years. Patient age and cancer type were not associated with HIV status documentation in South Africa.</p><p><strong>Conclusion: </strong>Different cancer centers have different gaps in HIV status documentation and will require tailored strategies to improve processes for ascertaining and recording HIV-related information in cancer records. Further research by our consortium to identify opportunities for integrating HIV and cancer care delivery is underway.</p>","PeriodicalId":13568,"journal":{"name":"Infectious Agents and Cancer","volume":"18 1","pages":"65"},"PeriodicalIF":3.1000,"publicationDate":"2023-10-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10604780/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Agents and Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13027-023-00548-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: In East and Southern Africa, people with HIV (PWH) experience worse cancer-related outcomes and are at higher risk of developing certain cancers. Siloed care delivery pathways pose a substantial barrier to co-management of HIV and cancer care delivery.
Methods: We conducted cross-sectional studies of adult cancer patients at public radiotherapy and oncology units in Malawi (Kamuzu Central Hospital), Zimbabwe (Parirenyatwa Group of Hospitals), and South Africa (Charlotte Maxeke Hospital) between 2018 and 2019. We abstracted cancer- and HIV-related data from new cancer patient records and used Poisson regression with robust variance to identify patient characteristics associated with HIV documentation.
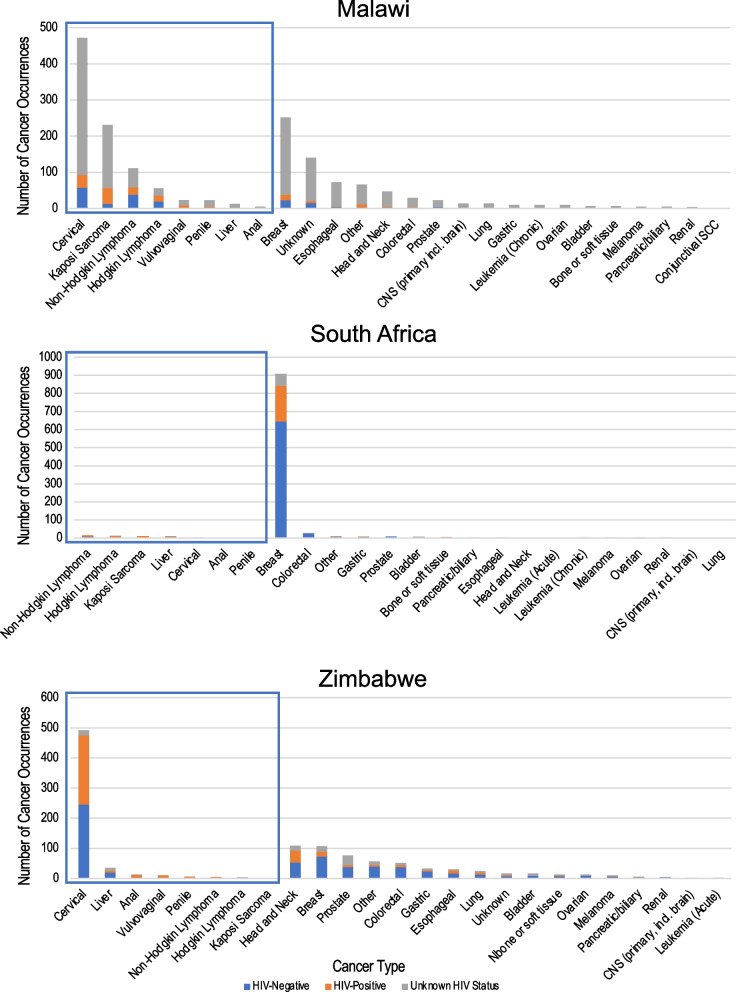
Results: We included 1,648 records from Malawi (median age 46 years), 1,044 records from South Africa (median age 55 years), and 1,135 records from Zimbabwe (median age 52 years). Records from all three sites were predominately from female patients; the most common cancers were cervical (Malawi [29%] and Zimbabwe [43%]) and breast (South Africa [87%]). HIV status was documented in 22% of cancer records from Malawi, 92% from South Africa, and 86% from Zimbabwe. Patients with infection-related cancers were more likely to have HIV status documented in Malawi (adjusted prevalence ratio [aPR]: 1.92, 95% confidence interval [CI]: 1.56-2.38) and Zimbabwe (aPR: 1.16, 95%CI: 1.10-1.22). Patients aged ≥ 60 years were less likely to have HIV status documented (Malawi: aPR: 0.66, 95% CI: 0.50-0.87; Zimbabwe: aPR: 0.76, 95%CI: 0.72-0.81) than patients under age 40 years. Patient age and cancer type were not associated with HIV status documentation in South Africa.
Conclusion: Different cancer centers have different gaps in HIV status documentation and will require tailored strategies to improve processes for ascertaining and recording HIV-related information in cancer records. Further research by our consortium to identify opportunities for integrating HIV and cancer care delivery is underway.
期刊介绍:
Infectious Agents and Cancer is an open access, peer-reviewed online journal that encompasses all aspects of basic, clinical, epidemiological and translational research providing an insight into the association between chronic infections and cancer.
The journal welcomes submissions in the pathogen-related cancer areas and other related topics, in particular:
• HPV and anogenital cancers, as well as head and neck cancers;
• EBV and Burkitt lymphoma;
• HCV/HBV and hepatocellular carcinoma as well as lymphoproliferative diseases;
• HHV8 and Kaposi sarcoma;
• HTLV and leukemia;
• Cancers in Low- and Middle-income countries.
The link between infection and cancer has become well established over the past 50 years, and infection-associated cancer contribute up to 16% of cancers in developed countries and 33% in less developed countries.
Preventive vaccines have been developed for only two cancer-causing viruses, highlighting both the opportunity to prevent infection-associated cancers by vaccination and the gaps that remain before vaccines can be developed for other cancer-causing agents. These gaps are due to incomplete understanding of the basic biology, natural history, epidemiology of many of the pathogens that cause cancer, the mechanisms they exploit to cause cancer, and how to interrupt progression to cancer in human populations. Early diagnosis or identification of lesions at high risk of progression represent the current most critical research area of the field supported by recent advances in genomics and proteomics technologies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


