Reinier Cornelis Anthonius van Linschoten, Anouk Sjoukje Huberts, Nikki van Leeuwen, Jan Antonius Hazelzet, Janneke van der Woude, Rachel Louise West, Desirée van Noord
{"title":"Validity of the self-administered comorbidity questionnaire in patients with inflammatory bowel disease.","authors":"Reinier Cornelis Anthonius van Linschoten, Anouk Sjoukje Huberts, Nikki van Leeuwen, Jan Antonius Hazelzet, Janneke van der Woude, Rachel Louise West, Desirée van Noord","doi":"10.1177/17562848231202159","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The International Consortium for Health Outcomes Measurement has selected the self-administered comorbidity questionnaire (SCQ) to adjust case-mix when comparing outcomes of inflammatory bowel disease (IBD) treatment between healthcare providers. However, the SCQ has not been validated for use in IBD patients.</p><p><strong>Objectives: </strong>We assessed the validity of the SCQ for measuring comorbidities in IBD patients.</p><p><strong>Design: </strong>Cohort study.</p><p><strong>Methods: </strong>We assessed the criterion validity of the SCQ for IBD patients by comparing patient-reported and clinician-reported comorbidities (as noted in the electronic health record) of the 13 diseases of the SCQ using Cohen's kappa. Construct validity was assessed using the Spearman correlation coefficient between the SCQ and the Charlson Comorbidity Index (CCI), clinician-reported SCQ, quality of life, IBD-related healthcare and productivity costs, prevalence of disability, and IBD disease activity. We assessed responsiveness by correlating changes in the SCQ with changes in healthcare costs, productivity costs, quality of life, and disease activity after 15 months.</p><p><strong>Results: </strong>We included 613 patients. At least fair agreement (κ > 0.20) was found for most comorbidities, but the agreement was slight (κ < 0.20) for stomach disease [κ = 0.19, 95% CI (-0.03; 0.41)], blood disease [κ = 0.02, 95% CI (-0.06; 0.11)], and back pain [κ = 0.18, 95% CI (0.11; 0.25)]. Correlations were found between the SCQ and the clinician-reported SCQ [ρ = 0.60, 95% CI (0.55; 0.66)], CCI [ρ = 0.39, 95% CI (0.31; 0.45)], the prevalence of disability [ρ = 0.23, 95% CI (0.15; 0.32)], and quality of life [ρ = -0.30, 95% CI (-0.37; -0.22)], but not between the SCQ and healthcare or productivity costs or disease activity (|ρ| ⩽ 0.2). A change in the SCQ after 15 months was not correlated with a change in any of the outcomes.</p><p><strong>Conclusion: </strong>The SCQ is a valid tool for measuring comorbidity in IBD patients, but face and content validity should be improved before being used to correct case-mix differences.</p>","PeriodicalId":3,"journal":{"name":"ACS Applied Electronic Materials","volume":null,"pages":null},"PeriodicalIF":4.3000,"publicationDate":"2023-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5c/20/10.1177_17562848231202159.PMC10591493.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Electronic Materials","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848231202159","RegionNum":3,"RegionCategory":"材料科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"ENGINEERING, ELECTRICAL & ELECTRONIC","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The International Consortium for Health Outcomes Measurement has selected the self-administered comorbidity questionnaire (SCQ) to adjust case-mix when comparing outcomes of inflammatory bowel disease (IBD) treatment between healthcare providers. However, the SCQ has not been validated for use in IBD patients.
Objectives: We assessed the validity of the SCQ for measuring comorbidities in IBD patients.
Design: Cohort study.
Methods: We assessed the criterion validity of the SCQ for IBD patients by comparing patient-reported and clinician-reported comorbidities (as noted in the electronic health record) of the 13 diseases of the SCQ using Cohen's kappa. Construct validity was assessed using the Spearman correlation coefficient between the SCQ and the Charlson Comorbidity Index (CCI), clinician-reported SCQ, quality of life, IBD-related healthcare and productivity costs, prevalence of disability, and IBD disease activity. We assessed responsiveness by correlating changes in the SCQ with changes in healthcare costs, productivity costs, quality of life, and disease activity after 15 months.
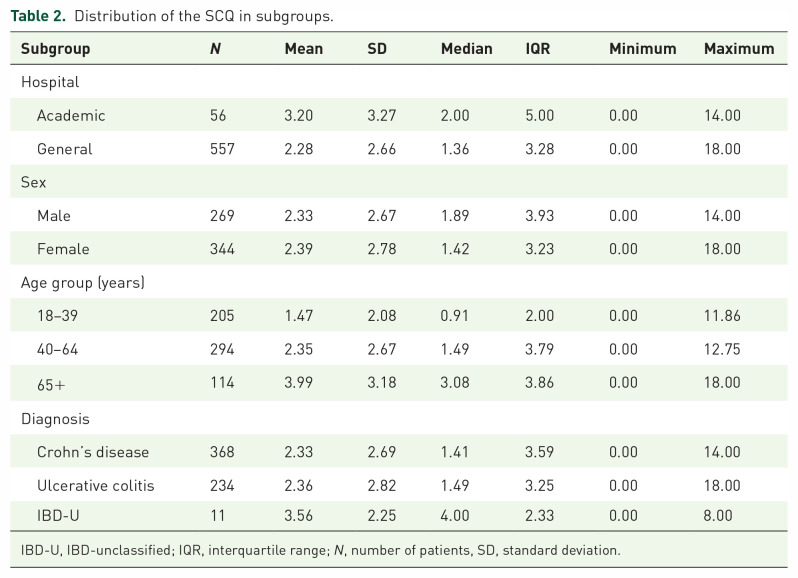
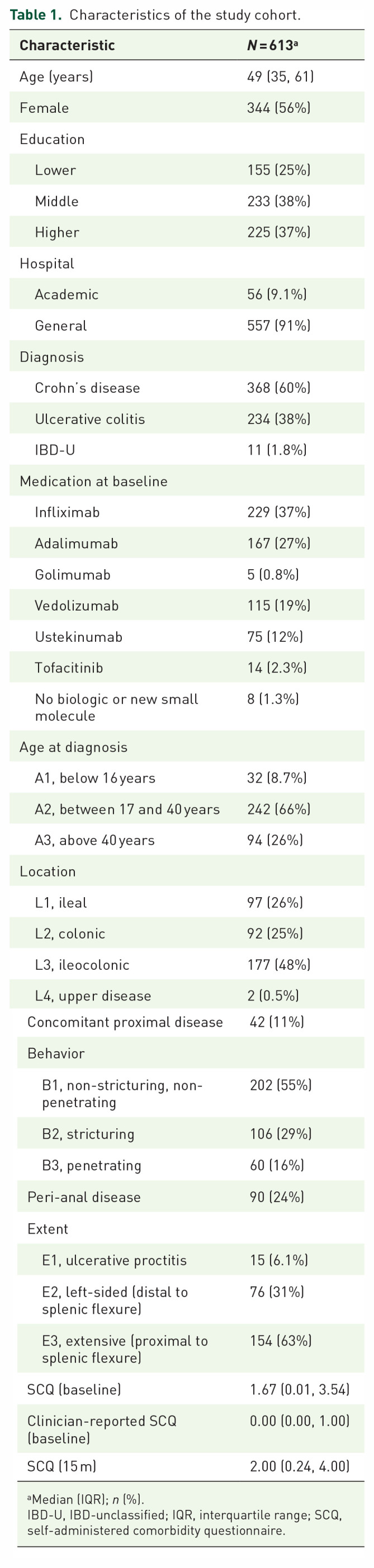
Results: We included 613 patients. At least fair agreement (κ > 0.20) was found for most comorbidities, but the agreement was slight (κ < 0.20) for stomach disease [κ = 0.19, 95% CI (-0.03; 0.41)], blood disease [κ = 0.02, 95% CI (-0.06; 0.11)], and back pain [κ = 0.18, 95% CI (0.11; 0.25)]. Correlations were found between the SCQ and the clinician-reported SCQ [ρ = 0.60, 95% CI (0.55; 0.66)], CCI [ρ = 0.39, 95% CI (0.31; 0.45)], the prevalence of disability [ρ = 0.23, 95% CI (0.15; 0.32)], and quality of life [ρ = -0.30, 95% CI (-0.37; -0.22)], but not between the SCQ and healthcare or productivity costs or disease activity (|ρ| ⩽ 0.2). A change in the SCQ after 15 months was not correlated with a change in any of the outcomes.
Conclusion: The SCQ is a valid tool for measuring comorbidity in IBD patients, but face and content validity should be improved before being used to correct case-mix differences.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


