Yisheng Peng, Hongwei Cheng, Hui Liu, Yang Zhang, Gang Liu
{"title":"Super-stable homogeneous embolic agents advance the treatment of hepatocellular carcinoma","authors":"Yisheng Peng, Hongwei Cheng, Hui Liu, Yang Zhang, Gang Liu","doi":"10.1002/ird3.22","DOIUrl":null,"url":null,"abstract":"<p>Hepatocellular carcinoma (HCC) is globally the sixth most prevalent and the third most fatal malignancy [<span>1</span>]. Although radical surgical resection is the optimal treatment strategy for HCC, it is not feasible for approximately 80% of HCC patients who present at intermediate or advanced stages [<span>2</span>]. Conversion therapy, particularly preoperative transcatheter arterial embolization/chemoembolization (TAE/TACE), enables unresectable HCC patients to undergo radical resection; this transition from palliative care to curative surgery enhances overall prognosis of HCC patients [<span>3</span>]. Many treatment guidelines recommend TACE as the first-line conversion therapy for patients with HCC [<span>4</span>]; however, its success rate remains low (11.9%–24.0%) [<span>5, 6</span>]. Traditional manual and three-way tube mixing methods for preparing iodized oil and drug emulsions are limited by the relatively low drug-loading capacity and poor physical stability of the hydrophobic iodized oil and hydrophilic drug formulations. As a result, the drugs are quickly released into circulation, leading to poor therapeutic effects and severe adverse events [<span>7, 8</span>]. The alternative method of drug-loaded microsphere embolization is costly and less effective due to microsphere size limitations [<span>9</span>]. Therefore, finding ways to improve the success rate of conversion therapy is a major challenge that needs to be urgently addressed.</p><p>The long-term survival of HCC patients relies on them undergoing radical surgical resection after successful conversion therapy. Despite postoperative, high-recurrence risk factors, such as large tumors, vascular invasion, metastases, and portal vein tumor thrombus, accurate surgical resection with no residual lesions has been shown to improve treatment efficacy in high-risk liver cancer patients [<span>4</span>]. Indocyanine green (ICG)-fluorescence-guided surgery can help to accurately determine tumor boundaries, identify small tumor metastases, and facilitate precise tumor resection [<span>10</span>]. Severe tumor necrosis and local inflammation caused by TACE conversion therapy markedly limit the operating space of laparoscopic surgery [<span>11, 12</span>]. In laparoscopic surgery without tactile feedback, sensitive fluorescence navigation technology greatly increases the precision of tumor resection [<span>13</span>]. However, because over 90% of the blood supplying liver lesions comes from the hepatic artery, interventional embolization conversion therapy leads to the destruction of almost all the tumor arterial blood supply [<span>14</span>]. Moreover, traditional fluorescence navigation methods cannot be effectively implemented intraoperatively as the fluorescent probes have difficulty accessing the tumor area [<span>12</span>]. Overcoming these obstacles and achieving precise liver tumor resection after conversion therapy is key to prolonging patient survival and reducing postoperative tumor recurrence.</p><p>The low conversion rate of liver cancer and the lack of highly sensitive molecular imaging probes after TACE surgery necessitate the development of novel approaches for sequential and precise surgical navigation during the transformational treatment of liver cancer. A super-stable homogeneous intermixed formulation technology (SHIFT) was developed to prepare homogeneous formulations of iodized oil and drugs under supercritical conditions to improve the efficacy of interventional therapy [<span>15</span>]. Super-stable homogeneous intermixed formulation technology mixes clinically used drugs, such as molecular imaging probes (e.g., ICG and methylene blue) and chemotherapy drugs (e.g., doxorubicin and platinum-based agents), with iodized oil to improve their stability and achieve uniform dispersal in the iodized oil; thus, SHIFT enhances the therapeutic efficacy of drugs through their sustained release at the tumor site (Figure 1). Doxorubicin is a hydrophilic chemotherapy drug which disperses poorly in iodized oil. However, a super-stable homogeneous formulation of nanostructured doxorubicin (nanoDOX) was reported to improve its dispersion in iodized oil [<span>7</span>]. NanoDOX is a carrier-free nanodrug, which is prepared using supercritical carbon dioxide fluid. It possesses a well-defined spherical structure, a small particle size (~100 nm), and a high contact angle with iodized oil; all of these features ensure its dispersibility within the iodized oil. Furthermore, the SHIFT nanoDOX formulation exhibits good sustained release performance (~50% of drug released in 7 days). Thus, SHIFT increases the dispersibility of hydrophilic chemotherapeutic drugs in iodized oil, and thus, prolongs drug retention time and improves the success rate of TACE-based conversion therapy. Of note, ethical approval has been obtained for the clinical evaluation of nanoDOX-based TACE and the implementation of SHIFT is expected to significantly improve the therapeutic efficacy of this conversion therapy while decreasing the associated adverse effects (clinical registration number: ChiCTR2100051591).</p><p>By destroying tumor blood vessels, TACE impedes the delivery of molecular imaging probes to tumor tissues/cells. This may be overcome with the SHIFT-based drug solubilization strategy, which can uniformly disperse the ICG formulation in iodized oil [<span>15</span>], improving the fluorescence stability and antifluorescence quenching capability of this probe. Because of the targeted delivery of fluorescent probes to the tumor by interventional therapy and specific deposition of iodized oil in tumor cells, ICG-iodized oil can effectively penetrate into tumor lesions. Findings from a clinical study (clinical registration number: ChiCTR2000035055) in which 45 patients with liver cancer were treated with a super-stable SHIFT-derived ICG formulation have recently been reported [<span>12</span>]. The fluorescence surgery navigation results showed an excellent level of tumor-specific deposition of ICG in patients confirming the feasibility of the combined fluorescence navigation strategy after long-term TAE. The patients treated with the SHIFT-derived ICG-iodized oil preparation had much clearer boundaries between their tumor and normal tissues during surgery than the patients who received the traditional intravenous injection of ICG after interventional therapy. Moreover, the SHIFT-derived ICG-iodized oil formulation helped surgeons in detecting microsatellite lesions, which had been missed before surgery. Thus, the SHIFT-based ICG formulation may overcome the shortcomings of ICG fluorescence navigation after conversion therapy and improve the efficacy of fluorescence navigation surgery for patients with advanced liver cancer.</p><p>Taking inspiration from the successful use of nanomaterials for drug delivery in cancer therapy, SHIFT is being developed further to prepare nanoformulations with unique physical and chemical properties [<span>16</span>]. For instance, SHIFT was used to prepare ICG nanoparticles (nanoICG) with a superior fluorescence imaging performance and antibleaching capability than conventional ICG. The enhanced permeability and retention effect of nanoparticles also enhance the tumor targeting capability of fluorescence dyes and improve their ability to detect small metastatic foci. The combination of pure drug nanotechnology and iodized oil embolization has shown encouraging results in primary tumor models. Moreover, the biosafety and fluorescence navigation performance of nanoICG were confirmed in the clinical case report (clinical registration number: ChiCTR2200058803). To overcome the low rate of successful conversion following TAE, a clinical interventional study was recently approved to determine the efficacy and safety of a sequential and precise surgical resection with SHIFT-assisted TACE (clinical registration number: ChiCTR2300070127). Early evidence suggests that SHIFT has great translational potential in improving the success rate of conversion therapy and preventing the recurrence and metastasis of liver cancer. Thus, encouraging outcomes are anticipated in future interventional studies of patients with advanced HCC.</p><p>Furthermore, new applications of SHIFT in the treatment of liver cancer are emerging. For instance, SHIFT is being explored in the sequential treatment of patients with liver cancer who are experiencing ruptured bleeding, leveraging its use in liver cancer embolization combined with fluorescence-guided surgery [<span>17</span>]. Moreover, in patients with liver metastasis from colorectal or pancreatic tumors, complete resection of all lesions is challenging due to the presence of multiple small tumor metastases [<span>18</span>]. Considering the sensitivity and specificity of ICG-iodized oil formulations in small tumor lesions, SHIFT may enable the detection of colorectal tumor liver metastasis and ensure precise tumor resection. In addition, SHIFT has shown promise when used in combination with transarterial radioembolization by improving the retention and stability of the radionuclide in the iodized oil. By improving the retention of the radionuclide within tumors, SHIFT acts as a one-stone-two-birds strategy, which enables the localized embolization and internal radiation of the tumor for imaging/therapeutic purposes [<span>19-21</span>]. SHIFT-derived radionuclide-iodized oil formulations allow embolic agent location monitoring and long-term radiation therapy, which may not be possible using conventional targeted radioactive microsphere therapy; however, ongoing research and development efforts will be necessary to address the drug-loading efficiency and pharmacokinetics of SHIFT-derived radionuclides-iodized oil formulations.</p><p>In summary, TAE-based sequential precision liver resection can effectively achieve long-term survival in patients with advanced liver cancer. Super-stable homogeneous intermixed formulation technology not only enhances the efficacy of TAE treatment by improving the dispersion of anticancer drugs in iodized oil but also facilitates precise tumor resection by delivering ICG to tumor sites through interventional embolization. Thus, SHIFT yields molecular imaging probes for liver resection after TAE, which can effectively navigate the complexities of advanced liver cancer. Furthermore, SHIFT also shows promise in the treatment of gastrointestinal tumors with liver metastasis. Notably, the properties of some traditional Chinese medicines and small molecule drugs restrict them to oral use or in vivo injection. The dispersion solubilization and granulation strategies based on the supercritical carbon dioxide technique used in SHIFT can improve the solubility of these drugs and expand their range of applications, ultimately enhancing their therapeutic efficacy. In the future, SHIFT will likely be subjected to further technological development and incorporate personalized medicine approaches in its implementation, with a focus on improving patient outcomes and expanding the clinical applications of this promising drug development strategy, especially in TAE-based sequential curative therapy.</p><p><b>Yisheng Peng</b>: Writing –original manuscript (lead). <b>Hongwei Cheng</b>: Writing –original manuscript. <b>Hui Liu</b>: Writing– review & editing (equal). <b>Yang Zhang</b>: Writing– review & editing (equal). <b>Gang Liu</b>: Writing – review & editing (lead).</p><p>Gang Liu is an <i>iRadiology</i> editorial board member but was not involved in the editorial review of this manuscript or the decision to publish it in <i>iRadiology</i>. All other authors have no conflicts of interest to declare.</p><p>This article adheres to the relevant ethical guidelines.</p><p>Not applicable.</p>","PeriodicalId":73508,"journal":{"name":"iRadiology","volume":"1 2","pages":"190-194"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ird3.22","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"iRadiology","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ird3.22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Hepatocellular carcinoma (HCC) is globally the sixth most prevalent and the third most fatal malignancy [1]. Although radical surgical resection is the optimal treatment strategy for HCC, it is not feasible for approximately 80% of HCC patients who present at intermediate or advanced stages [2]. Conversion therapy, particularly preoperative transcatheter arterial embolization/chemoembolization (TAE/TACE), enables unresectable HCC patients to undergo radical resection; this transition from palliative care to curative surgery enhances overall prognosis of HCC patients [3]. Many treatment guidelines recommend TACE as the first-line conversion therapy for patients with HCC [4]; however, its success rate remains low (11.9%–24.0%) [5, 6]. Traditional manual and three-way tube mixing methods for preparing iodized oil and drug emulsions are limited by the relatively low drug-loading capacity and poor physical stability of the hydrophobic iodized oil and hydrophilic drug formulations. As a result, the drugs are quickly released into circulation, leading to poor therapeutic effects and severe adverse events [7, 8]. The alternative method of drug-loaded microsphere embolization is costly and less effective due to microsphere size limitations [9]. Therefore, finding ways to improve the success rate of conversion therapy is a major challenge that needs to be urgently addressed.
The long-term survival of HCC patients relies on them undergoing radical surgical resection after successful conversion therapy. Despite postoperative, high-recurrence risk factors, such as large tumors, vascular invasion, metastases, and portal vein tumor thrombus, accurate surgical resection with no residual lesions has been shown to improve treatment efficacy in high-risk liver cancer patients [4]. Indocyanine green (ICG)-fluorescence-guided surgery can help to accurately determine tumor boundaries, identify small tumor metastases, and facilitate precise tumor resection [10]. Severe tumor necrosis and local inflammation caused by TACE conversion therapy markedly limit the operating space of laparoscopic surgery [11, 12]. In laparoscopic surgery without tactile feedback, sensitive fluorescence navigation technology greatly increases the precision of tumor resection [13]. However, because over 90% of the blood supplying liver lesions comes from the hepatic artery, interventional embolization conversion therapy leads to the destruction of almost all the tumor arterial blood supply [14]. Moreover, traditional fluorescence navigation methods cannot be effectively implemented intraoperatively as the fluorescent probes have difficulty accessing the tumor area [12]. Overcoming these obstacles and achieving precise liver tumor resection after conversion therapy is key to prolonging patient survival and reducing postoperative tumor recurrence.
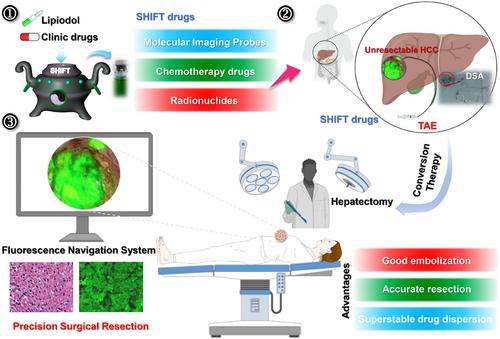
The low conversion rate of liver cancer and the lack of highly sensitive molecular imaging probes after TACE surgery necessitate the development of novel approaches for sequential and precise surgical navigation during the transformational treatment of liver cancer. A super-stable homogeneous intermixed formulation technology (SHIFT) was developed to prepare homogeneous formulations of iodized oil and drugs under supercritical conditions to improve the efficacy of interventional therapy [15]. Super-stable homogeneous intermixed formulation technology mixes clinically used drugs, such as molecular imaging probes (e.g., ICG and methylene blue) and chemotherapy drugs (e.g., doxorubicin and platinum-based agents), with iodized oil to improve their stability and achieve uniform dispersal in the iodized oil; thus, SHIFT enhances the therapeutic efficacy of drugs through their sustained release at the tumor site (Figure 1). Doxorubicin is a hydrophilic chemotherapy drug which disperses poorly in iodized oil. However, a super-stable homogeneous formulation of nanostructured doxorubicin (nanoDOX) was reported to improve its dispersion in iodized oil [7]. NanoDOX is a carrier-free nanodrug, which is prepared using supercritical carbon dioxide fluid. It possesses a well-defined spherical structure, a small particle size (~100 nm), and a high contact angle with iodized oil; all of these features ensure its dispersibility within the iodized oil. Furthermore, the SHIFT nanoDOX formulation exhibits good sustained release performance (~50% of drug released in 7 days). Thus, SHIFT increases the dispersibility of hydrophilic chemotherapeutic drugs in iodized oil, and thus, prolongs drug retention time and improves the success rate of TACE-based conversion therapy. Of note, ethical approval has been obtained for the clinical evaluation of nanoDOX-based TACE and the implementation of SHIFT is expected to significantly improve the therapeutic efficacy of this conversion therapy while decreasing the associated adverse effects (clinical registration number: ChiCTR2100051591).
By destroying tumor blood vessels, TACE impedes the delivery of molecular imaging probes to tumor tissues/cells. This may be overcome with the SHIFT-based drug solubilization strategy, which can uniformly disperse the ICG formulation in iodized oil [15], improving the fluorescence stability and antifluorescence quenching capability of this probe. Because of the targeted delivery of fluorescent probes to the tumor by interventional therapy and specific deposition of iodized oil in tumor cells, ICG-iodized oil can effectively penetrate into tumor lesions. Findings from a clinical study (clinical registration number: ChiCTR2000035055) in which 45 patients with liver cancer were treated with a super-stable SHIFT-derived ICG formulation have recently been reported [12]. The fluorescence surgery navigation results showed an excellent level of tumor-specific deposition of ICG in patients confirming the feasibility of the combined fluorescence navigation strategy after long-term TAE. The patients treated with the SHIFT-derived ICG-iodized oil preparation had much clearer boundaries between their tumor and normal tissues during surgery than the patients who received the traditional intravenous injection of ICG after interventional therapy. Moreover, the SHIFT-derived ICG-iodized oil formulation helped surgeons in detecting microsatellite lesions, which had been missed before surgery. Thus, the SHIFT-based ICG formulation may overcome the shortcomings of ICG fluorescence navigation after conversion therapy and improve the efficacy of fluorescence navigation surgery for patients with advanced liver cancer.
Taking inspiration from the successful use of nanomaterials for drug delivery in cancer therapy, SHIFT is being developed further to prepare nanoformulations with unique physical and chemical properties [16]. For instance, SHIFT was used to prepare ICG nanoparticles (nanoICG) with a superior fluorescence imaging performance and antibleaching capability than conventional ICG. The enhanced permeability and retention effect of nanoparticles also enhance the tumor targeting capability of fluorescence dyes and improve their ability to detect small metastatic foci. The combination of pure drug nanotechnology and iodized oil embolization has shown encouraging results in primary tumor models. Moreover, the biosafety and fluorescence navigation performance of nanoICG were confirmed in the clinical case report (clinical registration number: ChiCTR2200058803). To overcome the low rate of successful conversion following TAE, a clinical interventional study was recently approved to determine the efficacy and safety of a sequential and precise surgical resection with SHIFT-assisted TACE (clinical registration number: ChiCTR2300070127). Early evidence suggests that SHIFT has great translational potential in improving the success rate of conversion therapy and preventing the recurrence and metastasis of liver cancer. Thus, encouraging outcomes are anticipated in future interventional studies of patients with advanced HCC.
Furthermore, new applications of SHIFT in the treatment of liver cancer are emerging. For instance, SHIFT is being explored in the sequential treatment of patients with liver cancer who are experiencing ruptured bleeding, leveraging its use in liver cancer embolization combined with fluorescence-guided surgery [17]. Moreover, in patients with liver metastasis from colorectal or pancreatic tumors, complete resection of all lesions is challenging due to the presence of multiple small tumor metastases [18]. Considering the sensitivity and specificity of ICG-iodized oil formulations in small tumor lesions, SHIFT may enable the detection of colorectal tumor liver metastasis and ensure precise tumor resection. In addition, SHIFT has shown promise when used in combination with transarterial radioembolization by improving the retention and stability of the radionuclide in the iodized oil. By improving the retention of the radionuclide within tumors, SHIFT acts as a one-stone-two-birds strategy, which enables the localized embolization and internal radiation of the tumor for imaging/therapeutic purposes [19-21]. SHIFT-derived radionuclide-iodized oil formulations allow embolic agent location monitoring and long-term radiation therapy, which may not be possible using conventional targeted radioactive microsphere therapy; however, ongoing research and development efforts will be necessary to address the drug-loading efficiency and pharmacokinetics of SHIFT-derived radionuclides-iodized oil formulations.
In summary, TAE-based sequential precision liver resection can effectively achieve long-term survival in patients with advanced liver cancer. Super-stable homogeneous intermixed formulation technology not only enhances the efficacy of TAE treatment by improving the dispersion of anticancer drugs in iodized oil but also facilitates precise tumor resection by delivering ICG to tumor sites through interventional embolization. Thus, SHIFT yields molecular imaging probes for liver resection after TAE, which can effectively navigate the complexities of advanced liver cancer. Furthermore, SHIFT also shows promise in the treatment of gastrointestinal tumors with liver metastasis. Notably, the properties of some traditional Chinese medicines and small molecule drugs restrict them to oral use or in vivo injection. The dispersion solubilization and granulation strategies based on the supercritical carbon dioxide technique used in SHIFT can improve the solubility of these drugs and expand their range of applications, ultimately enhancing their therapeutic efficacy. In the future, SHIFT will likely be subjected to further technological development and incorporate personalized medicine approaches in its implementation, with a focus on improving patient outcomes and expanding the clinical applications of this promising drug development strategy, especially in TAE-based sequential curative therapy.
Gang Liu is an iRadiology editorial board member but was not involved in the editorial review of this manuscript or the decision to publish it in iRadiology. All other authors have no conflicts of interest to declare.
This article adheres to the relevant ethical guidelines.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


