{"title":"Stroke and systemic embolism in adult congenital heart disease","authors":"Katja Prokšelj","doi":"10.1016/j.ijcchd.2023.100453","DOIUrl":null,"url":null,"abstract":"<div><p>Despite striking improvement in survival of patients with congenital heart disease (CHD), the risk of long-term complications remains high. Stroke and systemic embolism are common and potentially devastating complications that significantly affect morbidity and mortality in CHD. The risk of stroke in adult congenital heart disease (ACHD) is higher than in the general population, patients are affected at an earlier age, and the risk continues to increase with age. Specific types of defects are at high-risk for stroke and other systemic embolisms, particularly patients with complex congenital heart disease, cyanotic heart disease, Fontan circulation, and cardiac shunts. Associated factors such as atrial arrhythmias, heart failure, mechanical valves and intracardiac devices, and infective endocarditis increase the risk of thromboembolic events. Acquired conventional risk factors for cardiovascular disease further increase the burden of stroke in the aging ACHD population. Anticoagulation is a cornerstone for prevention of thromboembolic events. Risk stratification in ACHD remains challenging and should be individualized. General risk stratification models, such as the CHA<sub>2</sub>DS<sub>2</sub>-VASc score, are not reliable in the heterogeneous ACHD population and should only be used in mild to moderate CHD. Anticoagulation is recommended as primary prevention in high-risk patients (patients with intracardiac repair, cyanotic CHD, Fontan circulation, or systemic right ventricle) with atrial arrhythmias. In patients with other CHD, general stratification models should be used to decide when to initiate anticoagulation, taking into account specificities of underlying heart disease and potential residua. Screening and treatment of conventional risk factors for cardiovascular disease may further improve long-term outcomes.</p></div>","PeriodicalId":73429,"journal":{"name":"International journal of cardiology. Congenital heart disease","volume":"12 ","pages":"Article 100453"},"PeriodicalIF":0.8000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International journal of cardiology. Congenital heart disease","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666668523000150","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 2
Abstract
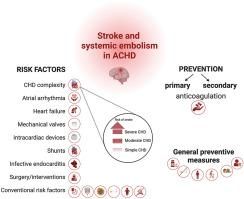
Despite striking improvement in survival of patients with congenital heart disease (CHD), the risk of long-term complications remains high. Stroke and systemic embolism are common and potentially devastating complications that significantly affect morbidity and mortality in CHD. The risk of stroke in adult congenital heart disease (ACHD) is higher than in the general population, patients are affected at an earlier age, and the risk continues to increase with age. Specific types of defects are at high-risk for stroke and other systemic embolisms, particularly patients with complex congenital heart disease, cyanotic heart disease, Fontan circulation, and cardiac shunts. Associated factors such as atrial arrhythmias, heart failure, mechanical valves and intracardiac devices, and infective endocarditis increase the risk of thromboembolic events. Acquired conventional risk factors for cardiovascular disease further increase the burden of stroke in the aging ACHD population. Anticoagulation is a cornerstone for prevention of thromboembolic events. Risk stratification in ACHD remains challenging and should be individualized. General risk stratification models, such as the CHA2DS2-VASc score, are not reliable in the heterogeneous ACHD population and should only be used in mild to moderate CHD. Anticoagulation is recommended as primary prevention in high-risk patients (patients with intracardiac repair, cyanotic CHD, Fontan circulation, or systemic right ventricle) with atrial arrhythmias. In patients with other CHD, general stratification models should be used to decide when to initiate anticoagulation, taking into account specificities of underlying heart disease and potential residua. Screening and treatment of conventional risk factors for cardiovascular disease may further improve long-term outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


