{"title":"Serum Creatinine and Amylase in Drain to Predict Pancreatic Fistula Risk after Pancreatoduodenectomy.","authors":"Yunda Song, Subo Zhang","doi":"10.1159/000533869","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The identification of patients with low risk of clinically relevant postoperative pancreatic fistula (CR-POPF) and postoperative hemorrhage (PPH) can guide drain removal after pancreatoduodenectomy (PD). However, drain fluid amylase (DFA) ≤5,000 U/L on postoperative day (POD) 1 does not robustly predict the absence of CR-POPF.</p><p><strong>Methods: </strong>Consecutive patients undergoing PD at Sun Yat-sen University Cancer Center between July 2018 and October 2021 were analyzed. Recursive partitioning analysis was used to classify patients into groups with different risks of CR-POPF and PPH.</p><p><strong>Results: </strong>Among 288 consecutive patients included, 99 patients (34.38%) developed CR-POPF (86 grade B and 13 grade C). Patients with CR-POPF had increased levels of preoperative creatinine (CRE) and POD1 CRE. The combination of POD1 CRE (>104 μmol/L or not) and POD1 DFA (>5,000 U/L or not) stratified patients into subgroups with the maximum difference in CR-POPF risk. The CR-POPF rates were 17.82% (36/202) in group A (POD1 CRE ≤104 μmol/L and POD1 DFA ≤5,000 U/L), 53.33% (8/15) in group B (POD1 CRE >104 μmol/L and POD1 DFA ≤5,000 U/L), and 77.46% (55/71) in group C (POD1 DFA >5,000 U/L). The PPH rates were 1.98% (4/202), 20.00% (3/15), and 19.72% (14/71) in groups A, B, and C, respectively.</p><p><strong>Conclusion: </strong>Patients with POD1 DFA ≤5,000 U/L and POD1 CRE >104 μmol/L have a high risk of CR-POPF and may not benefit from early drain removal. Patients with POD1 DFA ≤5,000 U/L and POD1 CRE ≤104 μmol/L have low risk of CR-POPF and PPH.</p>","PeriodicalId":11241,"journal":{"name":"Digestive Surgery","volume":" ","pages":"205-215"},"PeriodicalIF":1.2000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10716868/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000533869","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The identification of patients with low risk of clinically relevant postoperative pancreatic fistula (CR-POPF) and postoperative hemorrhage (PPH) can guide drain removal after pancreatoduodenectomy (PD). However, drain fluid amylase (DFA) ≤5,000 U/L on postoperative day (POD) 1 does not robustly predict the absence of CR-POPF.
Methods: Consecutive patients undergoing PD at Sun Yat-sen University Cancer Center between July 2018 and October 2021 were analyzed. Recursive partitioning analysis was used to classify patients into groups with different risks of CR-POPF and PPH.
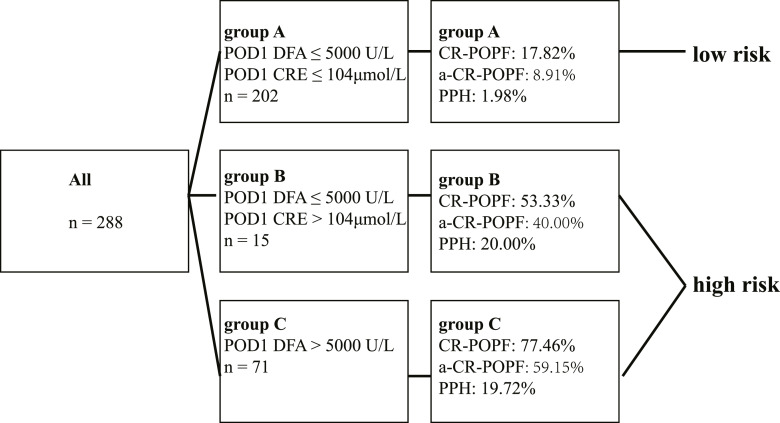
Results: Among 288 consecutive patients included, 99 patients (34.38%) developed CR-POPF (86 grade B and 13 grade C). Patients with CR-POPF had increased levels of preoperative creatinine (CRE) and POD1 CRE. The combination of POD1 CRE (>104 μmol/L or not) and POD1 DFA (>5,000 U/L or not) stratified patients into subgroups with the maximum difference in CR-POPF risk. The CR-POPF rates were 17.82% (36/202) in group A (POD1 CRE ≤104 μmol/L and POD1 DFA ≤5,000 U/L), 53.33% (8/15) in group B (POD1 CRE >104 μmol/L and POD1 DFA ≤5,000 U/L), and 77.46% (55/71) in group C (POD1 DFA >5,000 U/L). The PPH rates were 1.98% (4/202), 20.00% (3/15), and 19.72% (14/71) in groups A, B, and C, respectively.
Conclusion: Patients with POD1 DFA ≤5,000 U/L and POD1 CRE >104 μmol/L have a high risk of CR-POPF and may not benefit from early drain removal. Patients with POD1 DFA ≤5,000 U/L and POD1 CRE ≤104 μmol/L have low risk of CR-POPF and PPH.
期刊介绍:
''Digestive Surgery'' presents a comprehensive overview in the field of gastrointestinal surgery. Interdisciplinary in scope, the journal keeps the specialist aware of advances in all fields that contribute to improvements in the diagnosis and treatment of gastrointestinal disease. Particular emphasis is given to articles that evaluate not only recent clinical developments, especially clinical trials and technical innovations such as new endoscopic and laparoscopic procedures, but also relevant translational research. Each contribution is carefully aligned with the need of the digestive surgeon. Thus, the journal is an important component of the continuing medical education of surgeons who want their practice to benefit from a familiarity with new knowledge in all its dimensions.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


