Anders Aneman, Steven Frost, Michael Parr, Markus B Skrifvars
{"title":"Target temperature management following cardiac arrest: a systematic review and Bayesian meta-analysis.","authors":"Anders Aneman, Steven Frost, Michael Parr, Markus B Skrifvars","doi":"10.1186/s13054-022-03935-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Temperature control with target temperature management (TTM) after cardiac arrest has been endorsed by expert societies and adopted in international clinical practice guidelines but recent evidence challenges the use of hypothermic TTM.</p><p><strong>Methods: </strong>Systematic review and Bayesian meta-analysis of clinical trials on adult survivors from cardiac arrest undergoing TTM for at least 12 h comparing TTM versus no TTM or with a separation > 2 °C between intervention and control groups using the PubMed/MEDLINE, EMBASE, CENTRAL databases from inception to 1 September 2021 (PROSPERO CRD42021248140). All randomised and quasi-randomised controlled trials were considered. The risk ratio and 95% confidence interval for death (primary outcome) and unfavourable neurological recovery (secondary outcome) were captured using the original study definitions censored up to 180 days after cardiac arrest. Bias was assessed using the updated Cochrane risk-of-bias for randomised trials tool and certainty of evidence assessed using the Grading of Recommendation Assessment, Development and Evaluation methodology. A hierarchical robust Bayesian model-averaged meta-analysis was performed using both minimally informative and data-driven priors and reported by mean risk ratio (RR) and its 95% credible interval (95% CrI).</p><p><strong>Results: </strong>In seven studies (three low bias, three intermediate bias, one high bias, very low to low certainty) recruiting 3792 patients the RR by TTM 32-34 °C was 0.95 [95% CrI 0.78-1.09] for death and RR 0.93 [95% CrI 0.84-1.02] for unfavourable neurological outcome. The posterior probability for no benefit (RR ≥ 1) by TTM 32-34 °C was 24% for death and 12% for unfavourable neurological outcome. The posterior probabilities for favourable treatment effects of TTM 32-34 °C were the highest for an absolute risk reduction of 2-4% for death (28-53% chance) and unfavourable neurological outcome (63-78% chance). Excluding four studies without active avoidance of fever in the control arm reduced the probability to achieve an absolute risk reduction > 2% for death or unfavourable neurological outcome to ≤ 50%.</p><p><strong>Conclusions: </strong>The posterior probability distributions did not support the use of TTM at 32-34 °C compared to 36 °C also including active control of fever to reduce the risk of death and unfavourable neurological outcome at 90-180 days. Any likely benefit of hypothermic TTM is smaller than targeted in RCTs to date.</p>","PeriodicalId":92888,"journal":{"name":"Critical care (Houten, Netherlands)","volume":" ","pages":"58"},"PeriodicalIF":0.0000,"publicationDate":"2022-03-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8917746/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care (Houten, Netherlands)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13054-022-03935-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Temperature control with target temperature management (TTM) after cardiac arrest has been endorsed by expert societies and adopted in international clinical practice guidelines but recent evidence challenges the use of hypothermic TTM.
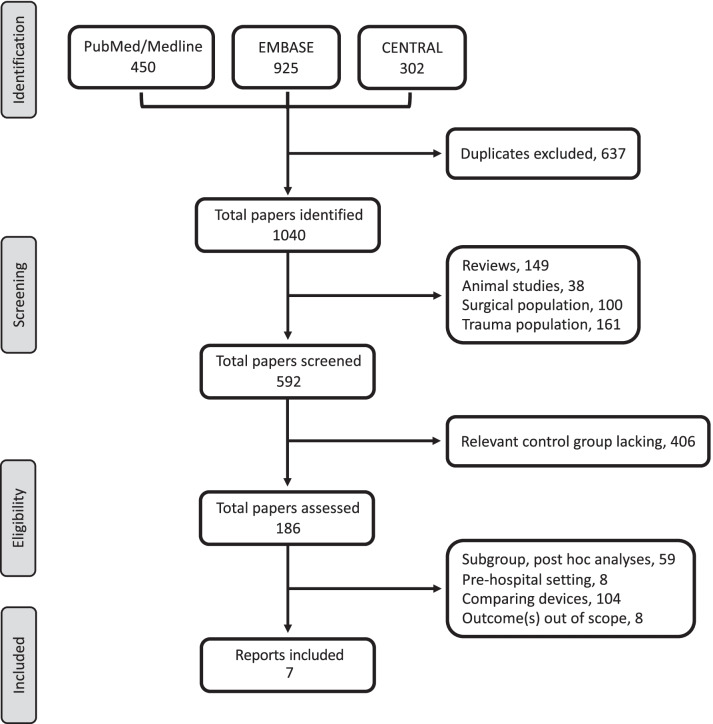
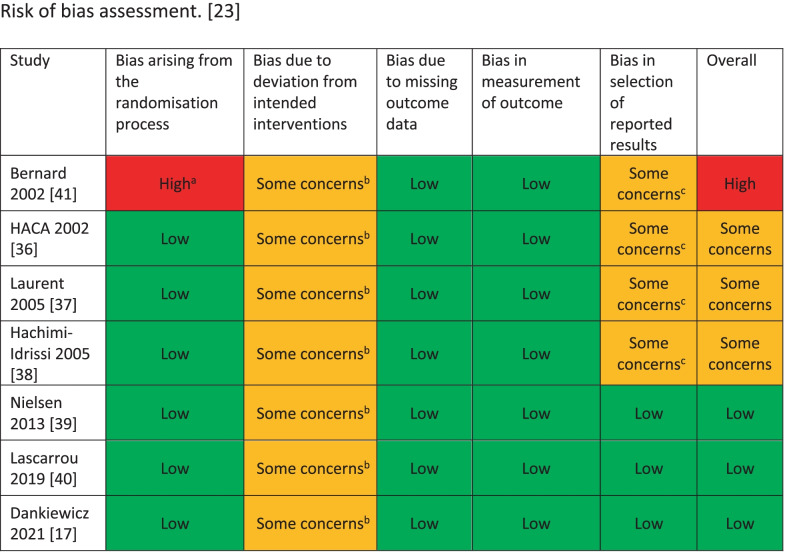
Methods: Systematic review and Bayesian meta-analysis of clinical trials on adult survivors from cardiac arrest undergoing TTM for at least 12 h comparing TTM versus no TTM or with a separation > 2 °C between intervention and control groups using the PubMed/MEDLINE, EMBASE, CENTRAL databases from inception to 1 September 2021 (PROSPERO CRD42021248140). All randomised and quasi-randomised controlled trials were considered. The risk ratio and 95% confidence interval for death (primary outcome) and unfavourable neurological recovery (secondary outcome) were captured using the original study definitions censored up to 180 days after cardiac arrest. Bias was assessed using the updated Cochrane risk-of-bias for randomised trials tool and certainty of evidence assessed using the Grading of Recommendation Assessment, Development and Evaluation methodology. A hierarchical robust Bayesian model-averaged meta-analysis was performed using both minimally informative and data-driven priors and reported by mean risk ratio (RR) and its 95% credible interval (95% CrI).
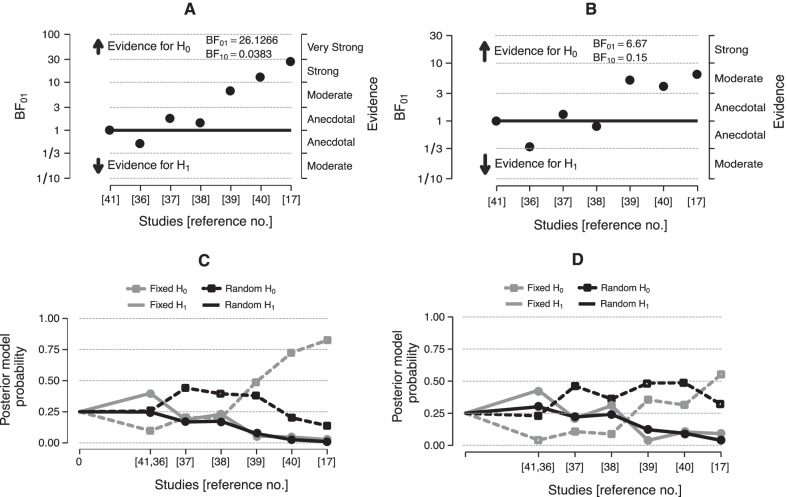
Results: In seven studies (three low bias, three intermediate bias, one high bias, very low to low certainty) recruiting 3792 patients the RR by TTM 32-34 °C was 0.95 [95% CrI 0.78-1.09] for death and RR 0.93 [95% CrI 0.84-1.02] for unfavourable neurological outcome. The posterior probability for no benefit (RR ≥ 1) by TTM 32-34 °C was 24% for death and 12% for unfavourable neurological outcome. The posterior probabilities for favourable treatment effects of TTM 32-34 °C were the highest for an absolute risk reduction of 2-4% for death (28-53% chance) and unfavourable neurological outcome (63-78% chance). Excluding four studies without active avoidance of fever in the control arm reduced the probability to achieve an absolute risk reduction > 2% for death or unfavourable neurological outcome to ≤ 50%.
Conclusions: The posterior probability distributions did not support the use of TTM at 32-34 °C compared to 36 °C also including active control of fever to reduce the risk of death and unfavourable neurological outcome at 90-180 days. Any likely benefit of hypothermic TTM is smaller than targeted in RCTs to date.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


