{"title":"Multicentre external validation of the GES score for predicting HCC risk in Japanese HCV patients who achieved SVR following DAAs","authors":"Kazumichi Abe, Masashi Fujita, Manabu Hayashi, Atsushi Takahashi, Hiromasa Ohira, Nabiel Mikhail, Reham Soliman, Gamal Shiha","doi":"10.1002/lci2.41","DOIUrl":null,"url":null,"abstract":"<p>A simple score combining clinical and biochemical parameters (general evaluation score (GES)) has shown value in predicting hepatocellular carcinoma (HCC) risk after hepatitis C virus (HCV) eradication in Egyptian patients with HCV genotype 4. We aimed to apply the GES to predict HCC risk in Japanese HCV patients who achieved sustained virological response (SVR) following direct-acting antivirals (DAAs). This multicentre retrospective cohort study included 187 HCV patients without a history of HCC treatment who achieved SVR. The GES was calculated using pre- and post-treatment data. The median age of the patients was 66 years; 49% were male, 89% had cirrhosis and 69% had HCV genotype 1. During the mean 36-month follow-up, 19 (10.2%) developed HCC. Regarding the pretreatment scores, 75 (40.1%), 58 (31.0%) and 54 (28.9%) patients had low-, intermediate- and high-risk scores, respectively. The 4-year cumulative incidence (CumI) was 1.64% in the low-risk group, 2.82% in the intermediate-risk group and 6.88% in the high-risk group (log-rank <i>P</i> = .029). In patients with cirrhosis, 60 (36.1%), 57 (34.3%) and 49 (29.5%) had low-, intermediate- and high-risk scores respectively. The 4-year CumI was 0.98% in the low-risk group, 2.86% in the intermediate-risk group and 6.67% in the high-risk group (log-rank <i>P</i> = .02). The GES calculated with pretreatment data was more useful than that calculated with post-treatment data (Harrell's C statistic: 0.670 vs 0.587). This tool incorporates changes over time to estimate variations in HCC risk and could help identify low-risk patients for whom HCC surveillance can be discontinued.</p>","PeriodicalId":93331,"journal":{"name":"Liver cancer international","volume":"2 3","pages":"102-109"},"PeriodicalIF":0.0000,"publicationDate":"2021-10-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/lci2.41","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Liver cancer international","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/lci2.41","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
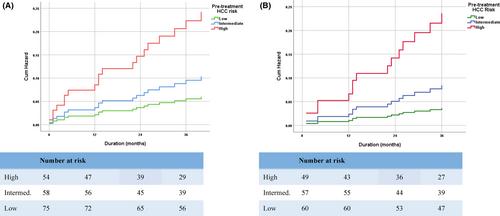
A simple score combining clinical and biochemical parameters (general evaluation score (GES)) has shown value in predicting hepatocellular carcinoma (HCC) risk after hepatitis C virus (HCV) eradication in Egyptian patients with HCV genotype 4. We aimed to apply the GES to predict HCC risk in Japanese HCV patients who achieved sustained virological response (SVR) following direct-acting antivirals (DAAs). This multicentre retrospective cohort study included 187 HCV patients without a history of HCC treatment who achieved SVR. The GES was calculated using pre- and post-treatment data. The median age of the patients was 66 years; 49% were male, 89% had cirrhosis and 69% had HCV genotype 1. During the mean 36-month follow-up, 19 (10.2%) developed HCC. Regarding the pretreatment scores, 75 (40.1%), 58 (31.0%) and 54 (28.9%) patients had low-, intermediate- and high-risk scores, respectively. The 4-year cumulative incidence (CumI) was 1.64% in the low-risk group, 2.82% in the intermediate-risk group and 6.88% in the high-risk group (log-rank P = .029). In patients with cirrhosis, 60 (36.1%), 57 (34.3%) and 49 (29.5%) had low-, intermediate- and high-risk scores respectively. The 4-year CumI was 0.98% in the low-risk group, 2.86% in the intermediate-risk group and 6.67% in the high-risk group (log-rank P = .02). The GES calculated with pretreatment data was more useful than that calculated with post-treatment data (Harrell's C statistic: 0.670 vs 0.587). This tool incorporates changes over time to estimate variations in HCC risk and could help identify low-risk patients for whom HCC surveillance can be discontinued.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


