The sit-to-stand test as a patient-centered functional outcome for critical care research: a pooled analysis of five international rehabilitation studies.
Heather K O'Grady, Lara Edbrooke, Christopher Farley, Sue Berney, Linda Denehy, Zudin Puthucheary, Michelle E Kho
{"title":"The sit-to-stand test as a patient-centered functional outcome for critical care research: a pooled analysis of five international rehabilitation studies.","authors":"Heather K O'Grady, Lara Edbrooke, Christopher Farley, Sue Berney, Linda Denehy, Zudin Puthucheary, Michelle E Kho","doi":"10.1186/s13054-022-04048-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>With ICU mortality rates decreasing, it is increasingly important to identify interventions to minimize functional impairments and improve outcomes for survivors. Simultaneously, we must identify robust patient-centered functional outcomes for our trials. Our objective was to investigate the clinimetric properties of a progression of three outcome measures, from strength to function.</p><p><strong>Methods: </strong>Adults (≥ 18 years) enrolled in five international ICU rehabilitation studies. Participants required ICU admission were mechanically ventilated and previously independent. Outcomes included two components of the Physical Function in ICU Test-scored (PFIT-s): knee extensor strength and assistance required to move from sit to stand (STS); the 30-s STS (30 s STS) test was the third outcome. We analyzed survivors at ICU and hospital discharge. We report participant demographics, baseline characteristics, and outcome data using descriptive statistics. Floor effects represented ≥ 15% of participants with minimum score and ceiling effects ≥ 15% with maximum score. We calculated the overall group difference score (hospital discharge score minus ICU discharge) for participants with paired assessments.</p><p><strong>Results: </strong>Of 451 participants, most were male (n = 278, 61.6%) with a median age between 60 and 66 years, a mean APACHE II score between 19 and 24, a median duration of mechanical ventilation between 4 and 8 days, ICU length of stay (LOS) between 7 and 11 days, and hospital LOS between 22 and 31 days. For knee extension, we observed a ceiling effect in 48.5% (160/330) of participants at ICU discharge and in 74.7% (115/154) at hospital discharge; the median [1st, 3rd quartile] PFIT-s difference score (n = 139) was 0 [0,1] (p < 0.05). For STS assistance, we observed a ceiling effect in 45.9% (150/327) at ICU discharge and in 77.5% (79/102) at hospital discharge; the median PFIT-s difference score (n = 87) was 1 [0, 2] (p < 0.05). For 30 s STS, we observed a floor effect in 15.0% (12/80) at ICU discharge but did not observe a floor or ceiling effect at hospital discharge. The median 30 s STS difference score (n = 54) was 3 [1, 6] (p < 0.05).</p><p><strong>Conclusion: </strong>Among three progressive outcome measures evaluated in this study, the 30 s STS test appears to have the most favorable clinimetric properties to assess function at ICU and hospital discharge in moderate to severely ill participants.</p>","PeriodicalId":92888,"journal":{"name":"Critical care (Houten, Netherlands)","volume":" ","pages":"175"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9195216/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care (Houten, Netherlands)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13054-022-04048-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: With ICU mortality rates decreasing, it is increasingly important to identify interventions to minimize functional impairments and improve outcomes for survivors. Simultaneously, we must identify robust patient-centered functional outcomes for our trials. Our objective was to investigate the clinimetric properties of a progression of three outcome measures, from strength to function.
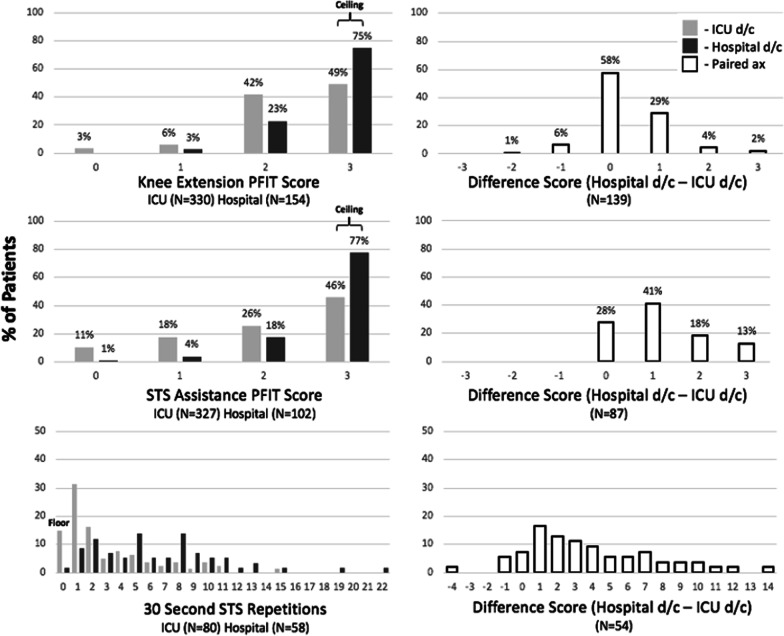
Methods: Adults (≥ 18 years) enrolled in five international ICU rehabilitation studies. Participants required ICU admission were mechanically ventilated and previously independent. Outcomes included two components of the Physical Function in ICU Test-scored (PFIT-s): knee extensor strength and assistance required to move from sit to stand (STS); the 30-s STS (30 s STS) test was the third outcome. We analyzed survivors at ICU and hospital discharge. We report participant demographics, baseline characteristics, and outcome data using descriptive statistics. Floor effects represented ≥ 15% of participants with minimum score and ceiling effects ≥ 15% with maximum score. We calculated the overall group difference score (hospital discharge score minus ICU discharge) for participants with paired assessments.
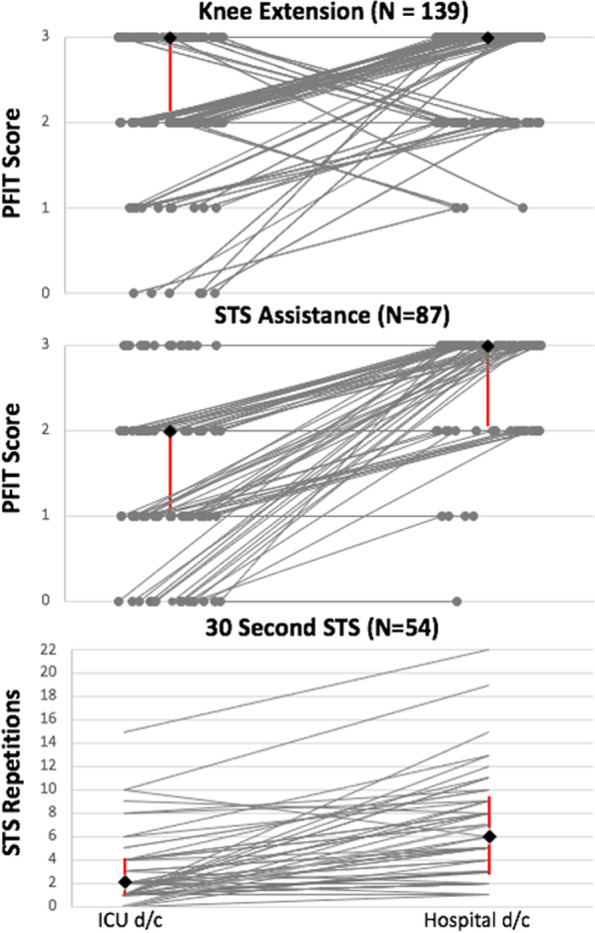
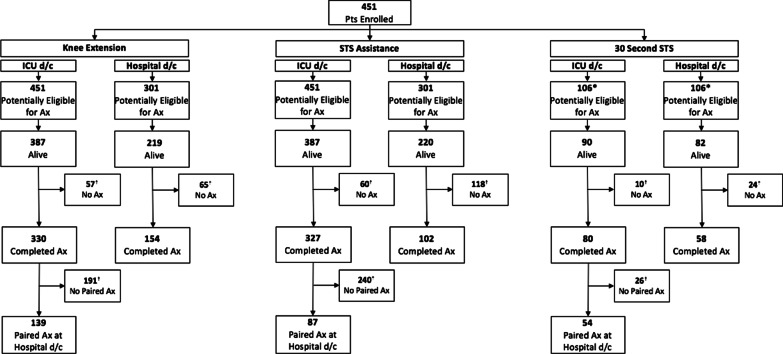
Results: Of 451 participants, most were male (n = 278, 61.6%) with a median age between 60 and 66 years, a mean APACHE II score between 19 and 24, a median duration of mechanical ventilation between 4 and 8 days, ICU length of stay (LOS) between 7 and 11 days, and hospital LOS between 22 and 31 days. For knee extension, we observed a ceiling effect in 48.5% (160/330) of participants at ICU discharge and in 74.7% (115/154) at hospital discharge; the median [1st, 3rd quartile] PFIT-s difference score (n = 139) was 0 [0,1] (p < 0.05). For STS assistance, we observed a ceiling effect in 45.9% (150/327) at ICU discharge and in 77.5% (79/102) at hospital discharge; the median PFIT-s difference score (n = 87) was 1 [0, 2] (p < 0.05). For 30 s STS, we observed a floor effect in 15.0% (12/80) at ICU discharge but did not observe a floor or ceiling effect at hospital discharge. The median 30 s STS difference score (n = 54) was 3 [1, 6] (p < 0.05).
Conclusion: Among three progressive outcome measures evaluated in this study, the 30 s STS test appears to have the most favorable clinimetric properties to assess function at ICU and hospital discharge in moderate to severely ill participants.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


