Progressing Towards Same-Day Discharges After Robotic-Assisted Radical Prostatectomy; Safe and Cost Effective to Discharge Without Routine Blood Tests.
Bodie Chislett, Ghadir Omran, Michael Harvey, Damien Bolton, Nathan Lawrentschuk
{"title":"Progressing Towards Same-Day Discharges After Robotic-Assisted Radical Prostatectomy; Safe and Cost Effective to Discharge Without Routine Blood Tests.","authors":"Bodie Chislett, Ghadir Omran, Michael Harvey, Damien Bolton, Nathan Lawrentschuk","doi":"10.2147/RRU.S429819","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Changing population demographics and the recent SARS-CoV-2 pandemic have forever changed healthcare, with increasing demands on straining systems. The economic cost is yet to be fully realised, with growing concerns around the current system's ability to accommodate the ageing comorbid population. Consequently, a paradigm shift has taken place in healthcare systems, prioritizing cost accountability. In the absence of established guidelines or robust literature, the use of laboratory tests postoperatively is often guided solely by clinician preference. This study presents a retrospective analysis that investigates the utility and cost implications of routine postoperative investigation following robotic-assisted radical prostatectomies. The findings aim to emphasise the importance of evidence-based practices and cost-effective approaches in postoperative care.</p><p><strong>Materials/methods: </strong>A retrospective analysis was performed on all robotic-assisted radical prostatectomies (RARP) identified from a single institution between 29th June 2017 to 28th June 2019. This interval was chosen in an attempt to avoid bias or confounding variables associated with the SRS-CoV-2 pandemic. A single clinician conducted a comprehensive medical record review using unit record numbers corresponding to identified procedural codes. Demographics and variables were recorded, including postoperative test results, hospital length of stay and 30-day readmission rates. Patients were assigned to either 'Routine Postoperative tests' (RPOT) or 'No Routine Postoperative tests' (No RPOT) and a comparative analysis was performed. Using the Australian National Pharmaceutical Benefits Scheme (PBS) pricing guide, total expenditure was calculated.</p><p><strong>Results: </strong>A total of 319 patients were included in the study with an average of 2.5 tests per patient within the first 24 hours. Routine postoperative tests had no bearing on outcomes, with comparable readmission rates between cohorts, and a significantly shorter length of stay in the \"No routine postoperative tests\" group when compared to the \"Routine Postoperative Tests\". A total of 1028 tests were performed within the first 48 hours following surgery with expenditure on routine testing totalling $20,516 based on the Australian PBS pricing schedule. Abnormal results were returned on 96% of patients. In the RPOT group, 18 out of the 20 common interventions occurred from 302 RARP. Among the patients in the RPOT group, eight individuals underwent blood transfusions. However, none of these patients met the hospital-specific criteria for transfusion, which require a hemoglobin level below 70 or symptomatic presentation with a hemoglobin level below 80.</p><p><strong>Conclusion: </strong>The data suggests routine postoperative laboratory has no bearing on re-admission rates, with patients experiencing significantly shorter hospital stays. Furthermore, our results indicate inefficient use of routine postoperative laboratory, with few clinical interventions, frequent abnormal results, and significant accumulative expenses.</p>","PeriodicalId":21008,"journal":{"name":"Research and Reports in Urology","volume":"15 ","pages":"471-477"},"PeriodicalIF":2.7000,"publicationDate":"2023-10-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8d/71/rru-15-471.PMC10575481.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Research and Reports in Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/RRU.S429819","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Changing population demographics and the recent SARS-CoV-2 pandemic have forever changed healthcare, with increasing demands on straining systems. The economic cost is yet to be fully realised, with growing concerns around the current system's ability to accommodate the ageing comorbid population. Consequently, a paradigm shift has taken place in healthcare systems, prioritizing cost accountability. In the absence of established guidelines or robust literature, the use of laboratory tests postoperatively is often guided solely by clinician preference. This study presents a retrospective analysis that investigates the utility and cost implications of routine postoperative investigation following robotic-assisted radical prostatectomies. The findings aim to emphasise the importance of evidence-based practices and cost-effective approaches in postoperative care.
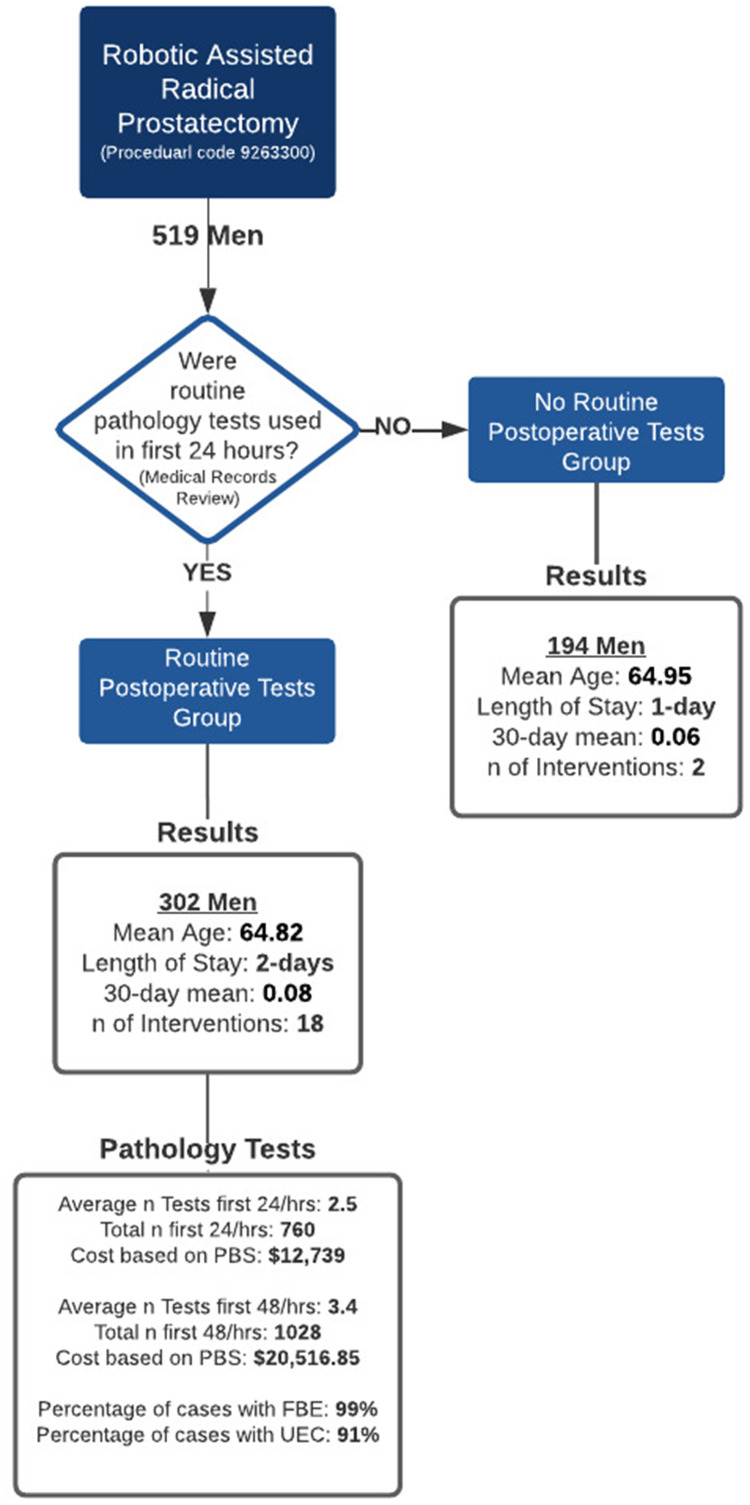
Materials/methods: A retrospective analysis was performed on all robotic-assisted radical prostatectomies (RARP) identified from a single institution between 29th June 2017 to 28th June 2019. This interval was chosen in an attempt to avoid bias or confounding variables associated with the SRS-CoV-2 pandemic. A single clinician conducted a comprehensive medical record review using unit record numbers corresponding to identified procedural codes. Demographics and variables were recorded, including postoperative test results, hospital length of stay and 30-day readmission rates. Patients were assigned to either 'Routine Postoperative tests' (RPOT) or 'No Routine Postoperative tests' (No RPOT) and a comparative analysis was performed. Using the Australian National Pharmaceutical Benefits Scheme (PBS) pricing guide, total expenditure was calculated.
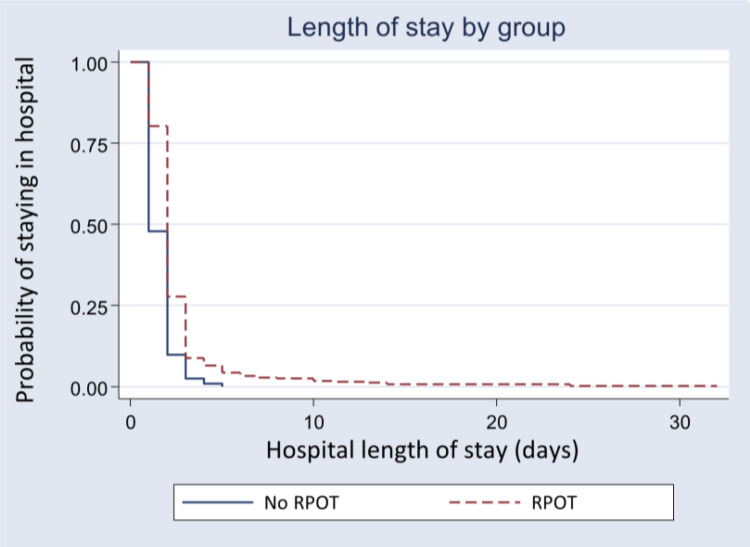
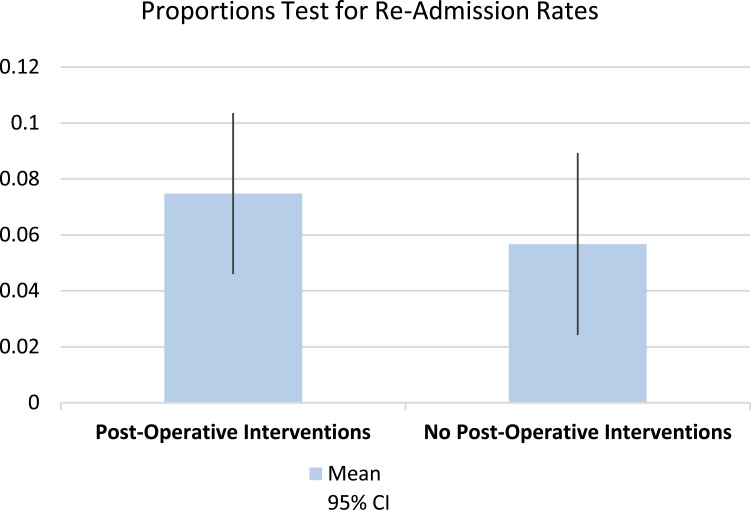
Results: A total of 319 patients were included in the study with an average of 2.5 tests per patient within the first 24 hours. Routine postoperative tests had no bearing on outcomes, with comparable readmission rates between cohorts, and a significantly shorter length of stay in the "No routine postoperative tests" group when compared to the "Routine Postoperative Tests". A total of 1028 tests were performed within the first 48 hours following surgery with expenditure on routine testing totalling $20,516 based on the Australian PBS pricing schedule. Abnormal results were returned on 96% of patients. In the RPOT group, 18 out of the 20 common interventions occurred from 302 RARP. Among the patients in the RPOT group, eight individuals underwent blood transfusions. However, none of these patients met the hospital-specific criteria for transfusion, which require a hemoglobin level below 70 or symptomatic presentation with a hemoglobin level below 80.
Conclusion: The data suggests routine postoperative laboratory has no bearing on re-admission rates, with patients experiencing significantly shorter hospital stays. Furthermore, our results indicate inefficient use of routine postoperative laboratory, with few clinical interventions, frequent abnormal results, and significant accumulative expenses.
期刊介绍:
Research and Reports in Urology is an international, peer-reviewed, open access, online journal. Publishing original research, reports, editorials, reviews and commentaries on all aspects of adult and pediatric urology in the clinic and laboratory including the following topics: Pathology, pathophysiology of urological disease Investigation and treatment of urological disease Pharmacology of drugs used for the treatment of urological disease Although the main focus of the journal is to publish research and clinical results in humans; preclinical, animal and in vitro studies will be published where they will shed light on disease processes and potential new therapies. Issues of patient safety and quality of care will also be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


