Prolonged Tracheal Intubation in the ICU as a Possible Risk Factor for Arytenoid Dislocation After Liver Transplant Surgery: A Retrospective Case-Control Study.
{"title":"Prolonged Tracheal Intubation in the ICU as a Possible Risk Factor for Arytenoid Dislocation After Liver Transplant Surgery: A Retrospective Case-Control Study.","authors":"Wenqing Yan, Weihua Dong, Zhi Chen","doi":"10.12659/AOT.940727","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Arytenoid dislocation (AD) is a rare complication of general anesthesia with tracheal intubation, with a published incidence of 0.009-0.097%. This retrospective case-control study aimed to identify risk factors associated with AD in patients who underwent liver transplantation. MATERIAL AND METHODS This study included 476 patients who underwent liver transplantation between January 2013 and December 2022. Patients with AD who underwent surgery were included in the AD group. For each case of AD, 4 patients matched by anesthesia type and anesthetist were randomly selected as the non-AD group. Data on patient characteristics, anesthetic factors, and surgical factors were collected and compared between patients with and without AD. Logistic regression analysis was performed to determine the risk factors for AD after liver transplantation. RESULTS Of the 476 patients who underwent liver transplantation, 17 (3.57%) had AD. AD occurred on the left side in 13 patients and on the right side in 4 patients. The 17 patients who experienced AD and 68 matched non-AD patients were enrolled. Patients in the AD group had a greater intubation depth (24 [23-24] vs 24 [24-24], P=0.043), a higher level of hemoglobin (134.5 [118-147.5] vs 112 [96.25-125], P=0.014), and prolonged tracheal intubation in the ICU (19.75 [15.87-31.87] vs 13 [10.62-15], P<0.001) compared to those in the non-dislocation group. Multivariate logistic regression analysis showed that prolonged tracheal intubation in the ICU was independently associated with the occurrence of AD in patients who underwent liver transplantation (P=0.013). CONCLUSIONS This study showed that the incidence of AD was 3.57% in patients undergoing liver transplant surgery and that prolonged tracheal intubation in the ICU was a possible risk factor for AD.</p>","PeriodicalId":7935,"journal":{"name":"Annals of Transplantation","volume":"28 ","pages":"e940727"},"PeriodicalIF":1.4000,"publicationDate":"2023-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8d/50/anntransplant-28-e940727.PMC10578641.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.12659/AOT.940727","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
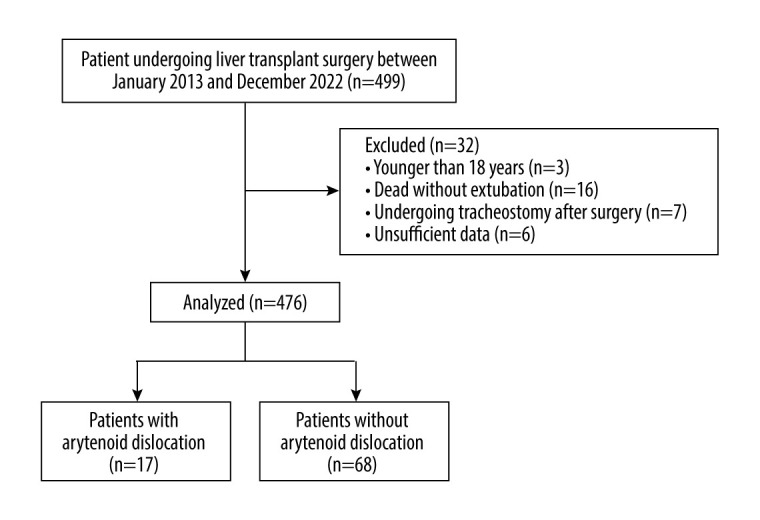
BACKGROUND Arytenoid dislocation (AD) is a rare complication of general anesthesia with tracheal intubation, with a published incidence of 0.009-0.097%. This retrospective case-control study aimed to identify risk factors associated with AD in patients who underwent liver transplantation. MATERIAL AND METHODS This study included 476 patients who underwent liver transplantation between January 2013 and December 2022. Patients with AD who underwent surgery were included in the AD group. For each case of AD, 4 patients matched by anesthesia type and anesthetist were randomly selected as the non-AD group. Data on patient characteristics, anesthetic factors, and surgical factors were collected and compared between patients with and without AD. Logistic regression analysis was performed to determine the risk factors for AD after liver transplantation. RESULTS Of the 476 patients who underwent liver transplantation, 17 (3.57%) had AD. AD occurred on the left side in 13 patients and on the right side in 4 patients. The 17 patients who experienced AD and 68 matched non-AD patients were enrolled. Patients in the AD group had a greater intubation depth (24 [23-24] vs 24 [24-24], P=0.043), a higher level of hemoglobin (134.5 [118-147.5] vs 112 [96.25-125], P=0.014), and prolonged tracheal intubation in the ICU (19.75 [15.87-31.87] vs 13 [10.62-15], P<0.001) compared to those in the non-dislocation group. Multivariate logistic regression analysis showed that prolonged tracheal intubation in the ICU was independently associated with the occurrence of AD in patients who underwent liver transplantation (P=0.013). CONCLUSIONS This study showed that the incidence of AD was 3.57% in patients undergoing liver transplant surgery and that prolonged tracheal intubation in the ICU was a possible risk factor for AD.
期刊介绍:
Annals of Transplantation is one of the fast-developing journals open to all scientists and fields of transplant medicine and related research. The journal is published quarterly and provides extensive coverage of the most important advances in transplantation.
Using an electronic on-line submission and peer review tracking system, Annals of Transplantation is committed to rapid review and publication. The average time to first decision is around 3-4 weeks. Time to publication of accepted manuscripts continues to be shortened, with the Editorial team committed to a goal of 3 months from acceptance to publication.
Expert reseachers and clinicians from around the world contribute original Articles, Review Papers, Case Reports and Special Reports in every pertinent specialty, providing a lot of arguments for discussion of exciting developments and controversies in the field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


