Defining longitudinal trajectory of body mass index percentile and predicting childhood obesity: methodologies and findings in the Boston Birth Cohort.
Wanyu Huang, Anat Yaskolka Meir, Bolanle Olapeju, Guoying Wang, Xiumei Hong, Maya Venkataramani, Tina L Cheng, Tak Igusa, Liming Liang, Xiaobin Wang
{"title":"Defining longitudinal trajectory of body mass index percentile and predicting childhood obesity: methodologies and findings in the Boston Birth Cohort.","authors":"Wanyu Huang, Anat Yaskolka Meir, Bolanle Olapeju, Guoying Wang, Xiumei Hong, Maya Venkataramani, Tina L Cheng, Tak Igusa, Liming Liang, Xiaobin Wang","doi":"10.1097/PN9.0000000000000037","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Overweight or obesity (OWO) in school-age childhood tends to persist into adulthood. This study aims to address a critical need for early identification of children at high risk of developing OWO by defining and analyzing longitudinal trajectories of body mass index percentile (BMIPCT) during early developmental windows.</p><p><strong>Methods: </strong>We included 3029 children from the Boston Birth Cohort (BBC) with repeated BMI measurements from birth to age 18 years. We applied locally weighted scatterplot smoothing with a time-limit scheme and predefined rules for imputation of missing data. We then used time-series <i>K</i>-means cluster analysis and latent class growth analysis to define longitudinal trajectories of BMIPCT from infancy up to age 18 years. Then, we investigated early life determinants of the BMI trajectories. Finally, we compared whether using early BMIPCT trajectories performs better than BMIPCT at a given age for predicting future risk of OWO.</p><p><strong>Results: </strong>After imputation, the percentage of missing data ratio decreased from 36.0% to 10.1%. We identified four BMIPCT longitudinal trajectories: early onset OWO; late onset OWO; normal stable; and low stable. Maternal OWO, smoking, and preterm birth were identified as important determinants of the two OWO trajectories. Our predictive models showed that BMIPCT trajectories in early childhood (birth to age 1 or 2 years) were more predictive of childhood OWO (age 5-10 years) than a single BMIPCT at age 1 or 2 years.</p><p><strong>Conclusions: </strong>Using longitudinal BMIPCT data from birth to age 18 years, this study identified distinct BMIPCT trajectories, examined early life determinants of these trajectories, and demonstrated their advantages in predicting childhood risk of OWO over BMIPCT at a single time point.</p>","PeriodicalId":74488,"journal":{"name":"Precision nutrition","volume":"2 2","pages":"e00037"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/22/e2/pn9-2-e00037.PMC10513013.pdf","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Precision nutrition","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/PN9.0000000000000037","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
Abstract
Background: Overweight or obesity (OWO) in school-age childhood tends to persist into adulthood. This study aims to address a critical need for early identification of children at high risk of developing OWO by defining and analyzing longitudinal trajectories of body mass index percentile (BMIPCT) during early developmental windows.
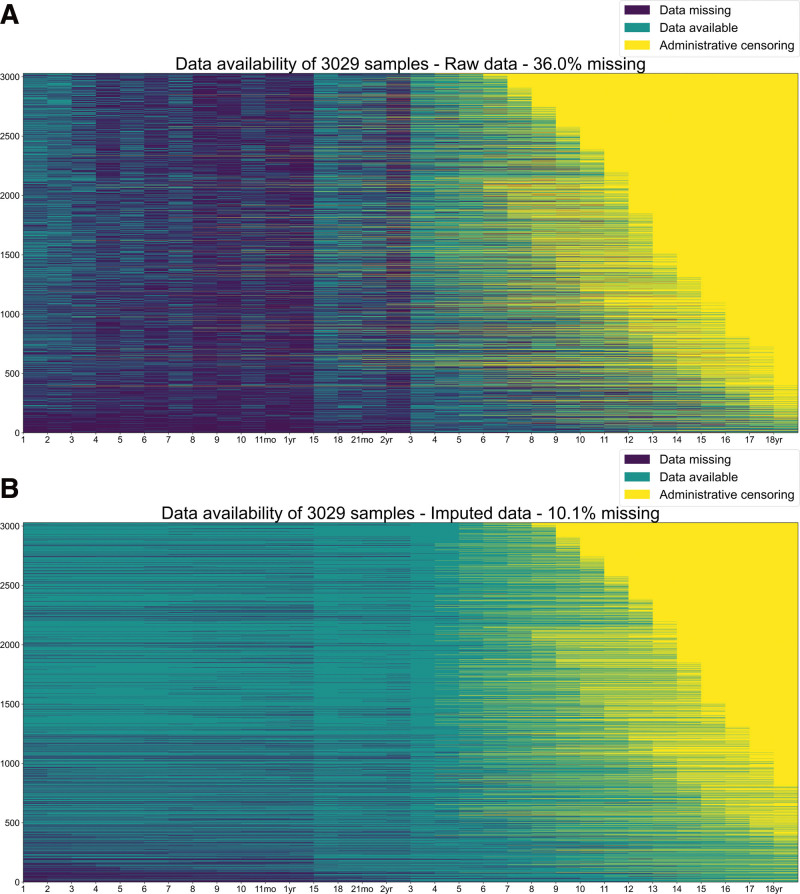
Methods: We included 3029 children from the Boston Birth Cohort (BBC) with repeated BMI measurements from birth to age 18 years. We applied locally weighted scatterplot smoothing with a time-limit scheme and predefined rules for imputation of missing data. We then used time-series K-means cluster analysis and latent class growth analysis to define longitudinal trajectories of BMIPCT from infancy up to age 18 years. Then, we investigated early life determinants of the BMI trajectories. Finally, we compared whether using early BMIPCT trajectories performs better than BMIPCT at a given age for predicting future risk of OWO.
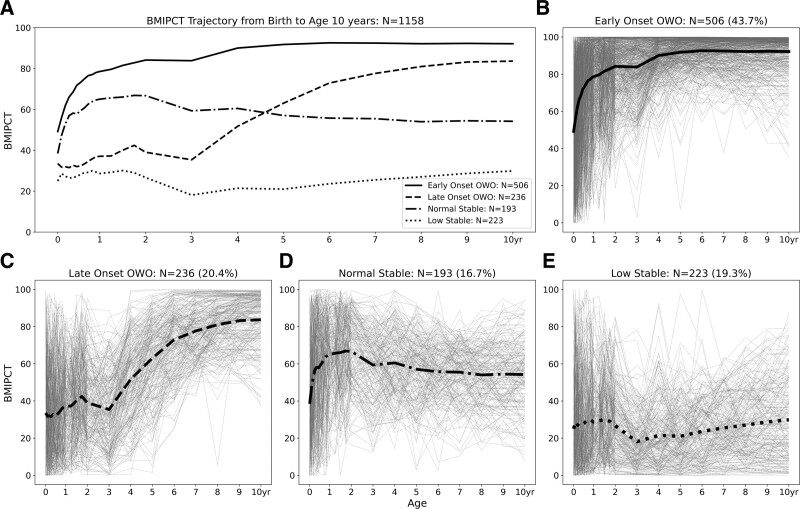
Results: After imputation, the percentage of missing data ratio decreased from 36.0% to 10.1%. We identified four BMIPCT longitudinal trajectories: early onset OWO; late onset OWO; normal stable; and low stable. Maternal OWO, smoking, and preterm birth were identified as important determinants of the two OWO trajectories. Our predictive models showed that BMIPCT trajectories in early childhood (birth to age 1 or 2 years) were more predictive of childhood OWO (age 5-10 years) than a single BMIPCT at age 1 or 2 years.
Conclusions: Using longitudinal BMIPCT data from birth to age 18 years, this study identified distinct BMIPCT trajectories, examined early life determinants of these trajectories, and demonstrated their advantages in predicting childhood risk of OWO over BMIPCT at a single time point.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


