Jorge Mariscal-Harana, Clint Asher, Vittoria Vergani, Maleeha Rizvi, Louise Keehn, Raymond J Kim, Robert M Judd, Steffen E Petersen, Reza Razavi, Andrew P King, Bram Ruijsink, Esther Puyol-Antón
{"title":"An artificial intelligence tool for automated analysis of large-scale unstructured clinical cine cardiac magnetic resonance databases.","authors":"Jorge Mariscal-Harana, Clint Asher, Vittoria Vergani, Maleeha Rizvi, Louise Keehn, Raymond J Kim, Robert M Judd, Steffen E Petersen, Reza Razavi, Andrew P King, Bram Ruijsink, Esther Puyol-Antón","doi":"10.1093/ehjdh/ztad044","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Artificial intelligence (AI) techniques have been proposed for automating analysis of short-axis (SAX) cine cardiac magnetic resonance (CMR), but no CMR analysis tool exists to automatically analyse large (unstructured) clinical CMR datasets. We develop and validate a robust AI tool for start-to-end automatic quantification of cardiac function from SAX cine CMR in large clinical databases.</p><p><strong>Methods and results: </strong>Our pipeline for processing and analysing CMR databases includes automated steps to identify the correct data, robust image pre-processing, an AI algorithm for biventricular segmentation of SAX CMR and estimation of functional biomarkers, and automated post-analysis quality control to detect and correct errors. The segmentation algorithm was trained on 2793 CMR scans from two NHS hospitals and validated on additional cases from this dataset (<i>n</i> = 414) and five external datasets (<i>n</i> = 6888), including scans of patients with a range of diseases acquired at 12 different centres using CMR scanners from all major vendors. Median absolute errors in cardiac biomarkers were within the range of inter-observer variability: <8.4 mL (left ventricle volume), <9.2 mL (right ventricle volume), <13.3 g (left ventricular mass), and <5.9% (ejection fraction) across all datasets. Stratification of cases according to phenotypes of cardiac disease and scanner vendors showed good performance across all groups.</p><p><strong>Conclusion: </strong>We show that our proposed tool, which combines image pre-processing steps, a domain-generalizable AI algorithm trained on a large-scale multi-domain CMR dataset and quality control steps, allows robust analysis of (clinical or research) databases from multiple centres, vendors, and cardiac diseases. This enables translation of our tool for use in fully automated processing of large multi-centre databases.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"4 5","pages":"370-383"},"PeriodicalIF":3.9000,"publicationDate":"2023-07-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10545512/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztad044","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: Artificial intelligence (AI) techniques have been proposed for automating analysis of short-axis (SAX) cine cardiac magnetic resonance (CMR), but no CMR analysis tool exists to automatically analyse large (unstructured) clinical CMR datasets. We develop and validate a robust AI tool for start-to-end automatic quantification of cardiac function from SAX cine CMR in large clinical databases.
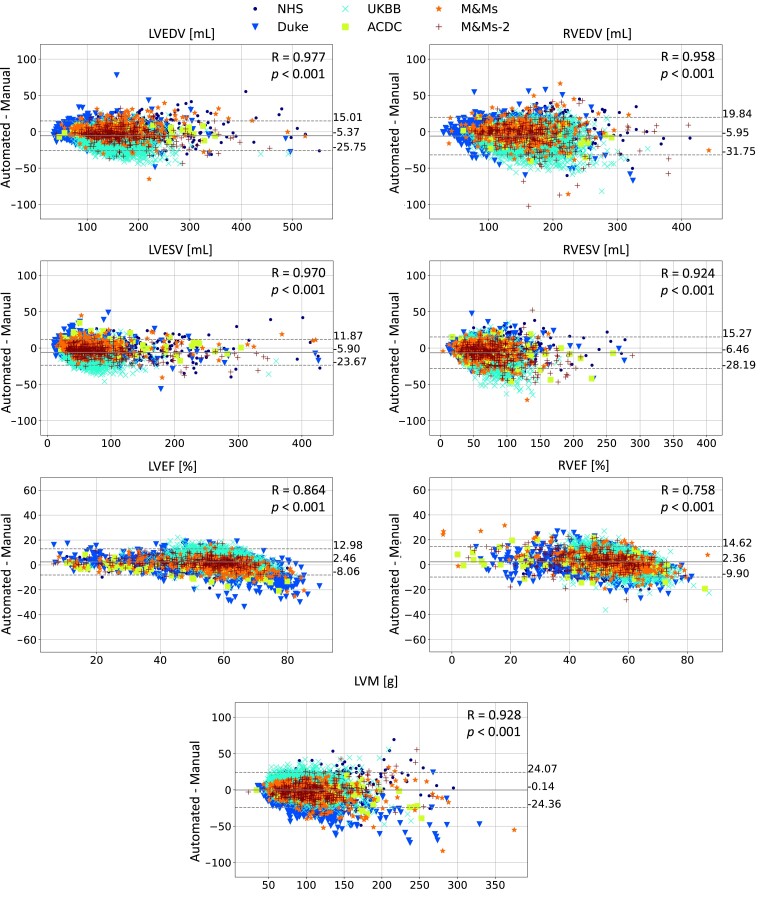
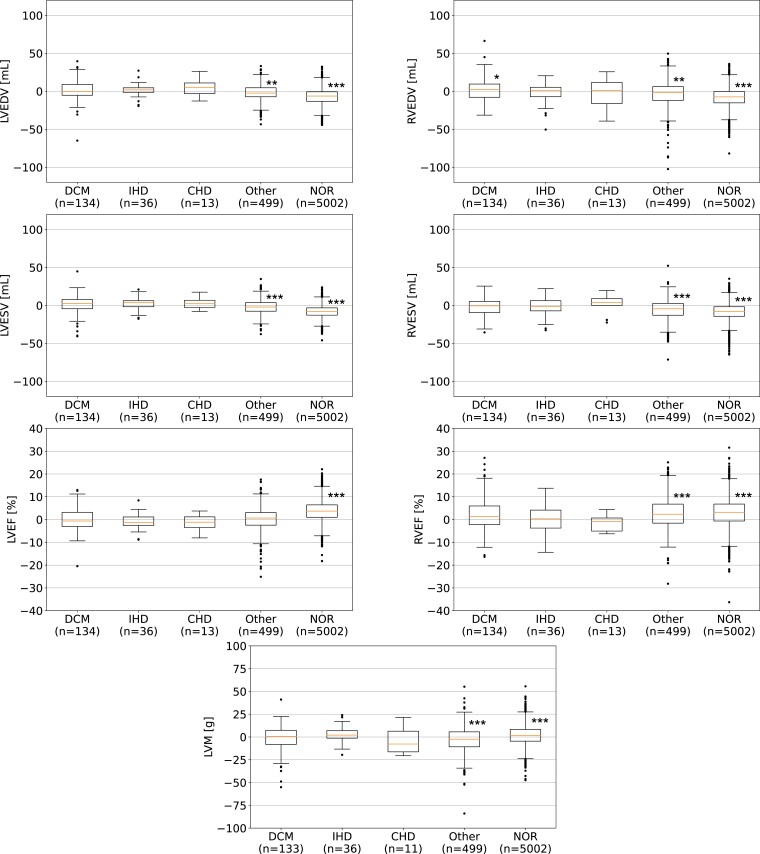
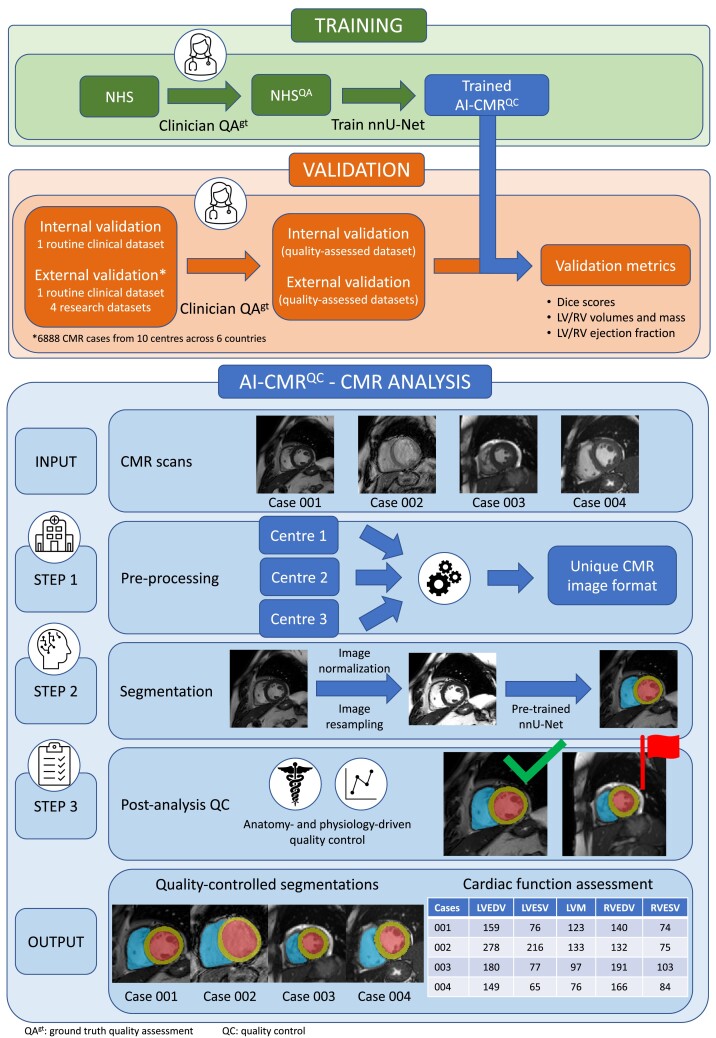
Methods and results: Our pipeline for processing and analysing CMR databases includes automated steps to identify the correct data, robust image pre-processing, an AI algorithm for biventricular segmentation of SAX CMR and estimation of functional biomarkers, and automated post-analysis quality control to detect and correct errors. The segmentation algorithm was trained on 2793 CMR scans from two NHS hospitals and validated on additional cases from this dataset (n = 414) and five external datasets (n = 6888), including scans of patients with a range of diseases acquired at 12 different centres using CMR scanners from all major vendors. Median absolute errors in cardiac biomarkers were within the range of inter-observer variability: <8.4 mL (left ventricle volume), <9.2 mL (right ventricle volume), <13.3 g (left ventricular mass), and <5.9% (ejection fraction) across all datasets. Stratification of cases according to phenotypes of cardiac disease and scanner vendors showed good performance across all groups.
Conclusion: We show that our proposed tool, which combines image pre-processing steps, a domain-generalizable AI algorithm trained on a large-scale multi-domain CMR dataset and quality control steps, allows robust analysis of (clinical or research) databases from multiple centres, vendors, and cardiac diseases. This enables translation of our tool for use in fully automated processing of large multi-centre databases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


