Ana Mendieta, Ligia Rios Lopez, Maria Vargas Arteaga, Essy Maradiegue, Walter Delgadillo Arone, Carlos Rueda Bazalar, Alexis Holguin, Carlos Santillan Salas, Ivan Maza, Maysam Homsi, Frankly Farias Barrios, Claudia Assayag, Liliana Vásquez, Claudia Pascual, Miguela Caniza
{"title":"A multimodal strategy to improve health care for pediatric patients with cancer and fever in Peru.","authors":"Ana Mendieta, Ligia Rios Lopez, Maria Vargas Arteaga, Essy Maradiegue, Walter Delgadillo Arone, Carlos Rueda Bazalar, Alexis Holguin, Carlos Santillan Salas, Ivan Maza, Maysam Homsi, Frankly Farias Barrios, Claudia Assayag, Liliana Vásquez, Claudia Pascual, Miguela Caniza","doi":"10.26633/RPSP.2023.140","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The DoTT (Decreasing Time to Therapy) project aimed to minimize the interval between fever onset and medical interventions for children with febrile neutropenia. The objective of this study was to determine the effect of implementing the DoTT project on the hospital time to antibiotic (TTA) and patient time to arrival (PTA) at the hospital in children with febrile neutropenia admitted to the emergency department.</p><p><strong>Methods: </strong>The DoTT project was implemented at a Peruvian hospital and followed the World Health Organization (WHO) multimodal improvement strategy model. Components included creating a healthcare delivery bundle and antibiotic selection pathways, training users of the bundle and pathways, monitoring patient outcomes and obtaining user feedback, encouraging use of the new system, and promoting the integration of DoTT into the institutional culture. Emergency room providers were trained in the care delivery for children with cancer and fever and taught to use the bundle and pathways. DoTT was promoted via pamphlets and posters, with a view to institutionalizing the concept and disseminating it to other hospital services.</p><p><strong>Results: </strong>Admission data for 129 eligible patients in our registry were analyzed. The TTA and PTA were compared before and after the DoTT intervention. The median TTA was 146 minutes (interquartile range [IQR] 97-265 minutes) before the intervention in 99 patients, and 69 minutes (IQR 50-120 minutes) afterwards in 30 patients (<i>p</i> < 0.01). The median PTA was reduced from 1 483 minutes at baseline to 660 minutes after the intervention (<i>p</i> < 0.01).</p><p><strong>Conclusions: </strong>Applying the WHO multimodal improvement strategy model to the care of children with febrile neutropenia arriving at the hospital had a positive impact on the PTA and TTA, thus potentially increasing the survival of these patients.</p>","PeriodicalId":21264,"journal":{"name":"Revista Panamericana De Salud Publica-pan American Journal of Public Health","volume":"47 ","pages":"e140"},"PeriodicalIF":2.0000,"publicationDate":"2023-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/41/43/rpsp-47-e140.PMC10548892.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista Panamericana De Salud Publica-pan American Journal of Public Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.26633/RPSP.2023.140","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The DoTT (Decreasing Time to Therapy) project aimed to minimize the interval between fever onset and medical interventions for children with febrile neutropenia. The objective of this study was to determine the effect of implementing the DoTT project on the hospital time to antibiotic (TTA) and patient time to arrival (PTA) at the hospital in children with febrile neutropenia admitted to the emergency department.
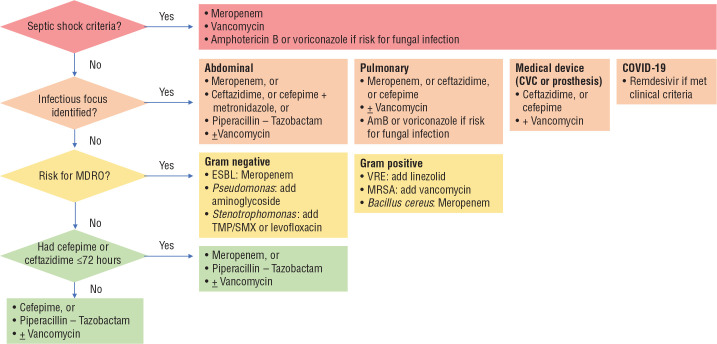
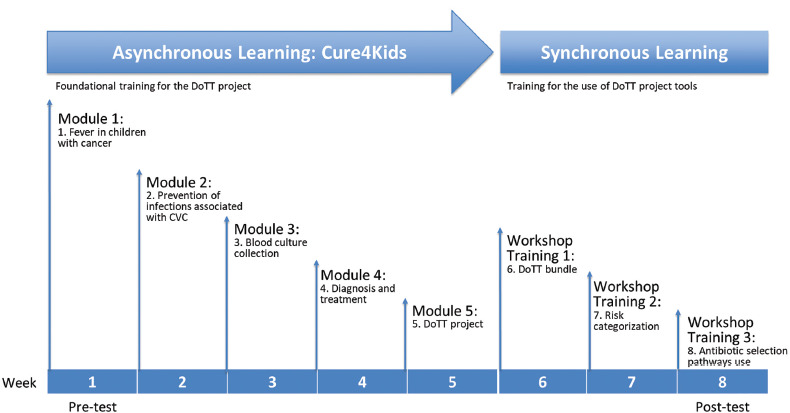
Methods: The DoTT project was implemented at a Peruvian hospital and followed the World Health Organization (WHO) multimodal improvement strategy model. Components included creating a healthcare delivery bundle and antibiotic selection pathways, training users of the bundle and pathways, monitoring patient outcomes and obtaining user feedback, encouraging use of the new system, and promoting the integration of DoTT into the institutional culture. Emergency room providers were trained in the care delivery for children with cancer and fever and taught to use the bundle and pathways. DoTT was promoted via pamphlets and posters, with a view to institutionalizing the concept and disseminating it to other hospital services.
Results: Admission data for 129 eligible patients in our registry were analyzed. The TTA and PTA were compared before and after the DoTT intervention. The median TTA was 146 minutes (interquartile range [IQR] 97-265 minutes) before the intervention in 99 patients, and 69 minutes (IQR 50-120 minutes) afterwards in 30 patients (p < 0.01). The median PTA was reduced from 1 483 minutes at baseline to 660 minutes after the intervention (p < 0.01).
Conclusions: Applying the WHO multimodal improvement strategy model to the care of children with febrile neutropenia arriving at the hospital had a positive impact on the PTA and TTA, thus potentially increasing the survival of these patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


