Ankit Bhardwaj, Hara Prasad Mishra, Ayush Goel, Ashi Gupta
{"title":"COVID-19 - a potential trigger for MOGAD-associated optic neuritis: a case report and literature review.","authors":"Ankit Bhardwaj, Hara Prasad Mishra, Ayush Goel, Ashi Gupta","doi":"10.1177/25158414231199541","DOIUrl":null,"url":null,"abstract":"<p><p>SARS-CoV-2 affects the nervous system directly by neurotoxic action, by binding to angiotensin-converting enzyme-2 (ACE2) receptors or indirectly by inducing cytokine storm leading to disruption of the blood-brain barrier, immunological mediation, increasing blood coagulation and as a trigger for autoimmune-mediated demyelinating injuries in the central nervous system. In COVID-19 neuro-ophthalmological manifestations are not so common. Optic neuritis is the result of optic nerve inflammation and has varied causes. In many patients, signs of inflammation are not visible on the fundus, and it usually manifests as papillitis-anterior neuritis, retrobulbar neuritis or visible optic nerve oedema. We are reporting a case of a middle-aged adult diagnosed with myelin oligodendrocyte glycoprotein (MOG) antibody-positive optic neuritis of the right eye post-COVID-19 disease. Routine biochemical and haematological investigations, including electrolytes and hepatic and renal functions, were normal. In cerebrospinal fluid (CSF) - glucose 63.8 mg/dL, protein 39.1 mg/dL and ADA - 1 µ/L. No oligoclonal bands of immunoglobulin G (IgG) were seen on high-resolution electrophoresis. Serum Anti-MOG-antibodies were positive. A gadolinium-contrast magnetic resonance imaging (MRI) of the brain and orbits shows post-contrast enhancement in the superior aspect of the right intraconal soft tissue. The right optic nerve appears bulky and heterogeneous with peripheral post-contrast enhancement along its entire length suggestive of neuritis. A diagnosis of MOG antibody-positive optic neuritis was made, and the patient was treated with an injection of Methylprednisolone with intravenous immunoglobulin. Each day, the evaluation of the right eye showed remarkable improvement from finger counting to 6/6 vision. The patient was discharged on the 9th day of admission. We can conclude that early diagnosis was essential for improving the long-term outcome of the patient.</p>","PeriodicalId":23054,"journal":{"name":"Therapeutic Advances in Ophthalmology","volume":"15 ","pages":"25158414231199541"},"PeriodicalIF":2.3000,"publicationDate":"2023-10-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ca/b1/10.1177_25158414231199541.PMC10559697.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/25158414231199541","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
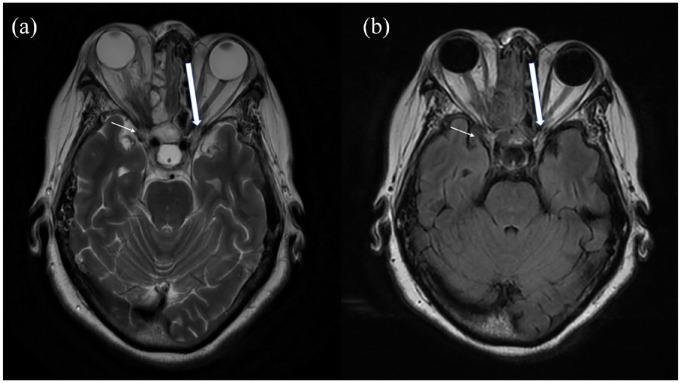
SARS-CoV-2 affects the nervous system directly by neurotoxic action, by binding to angiotensin-converting enzyme-2 (ACE2) receptors or indirectly by inducing cytokine storm leading to disruption of the blood-brain barrier, immunological mediation, increasing blood coagulation and as a trigger for autoimmune-mediated demyelinating injuries in the central nervous system. In COVID-19 neuro-ophthalmological manifestations are not so common. Optic neuritis is the result of optic nerve inflammation and has varied causes. In many patients, signs of inflammation are not visible on the fundus, and it usually manifests as papillitis-anterior neuritis, retrobulbar neuritis or visible optic nerve oedema. We are reporting a case of a middle-aged adult diagnosed with myelin oligodendrocyte glycoprotein (MOG) antibody-positive optic neuritis of the right eye post-COVID-19 disease. Routine biochemical and haematological investigations, including electrolytes and hepatic and renal functions, were normal. In cerebrospinal fluid (CSF) - glucose 63.8 mg/dL, protein 39.1 mg/dL and ADA - 1 µ/L. No oligoclonal bands of immunoglobulin G (IgG) were seen on high-resolution electrophoresis. Serum Anti-MOG-antibodies were positive. A gadolinium-contrast magnetic resonance imaging (MRI) of the brain and orbits shows post-contrast enhancement in the superior aspect of the right intraconal soft tissue. The right optic nerve appears bulky and heterogeneous with peripheral post-contrast enhancement along its entire length suggestive of neuritis. A diagnosis of MOG antibody-positive optic neuritis was made, and the patient was treated with an injection of Methylprednisolone with intravenous immunoglobulin. Each day, the evaluation of the right eye showed remarkable improvement from finger counting to 6/6 vision. The patient was discharged on the 9th day of admission. We can conclude that early diagnosis was essential for improving the long-term outcome of the patient.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


