The dichotomy of glucocorticosteroid treatment in immune-inflammatory rheumatic diseases: an evidence-based perspective and insights from clinical practice.
Elvis Hysa, Tamara Vojinovic, Emanuele Gotelli, Elisa Alessandri, Carmen Pizzorni, Sabrina Paolino, Alberto Sulli, Vanessa Smith, Maurizio Cutolo
{"title":"The dichotomy of glucocorticosteroid treatment in immune-inflammatory rheumatic diseases: an evidence-based perspective and insights from clinical practice.","authors":"Elvis Hysa, Tamara Vojinovic, Emanuele Gotelli, Elisa Alessandri, Carmen Pizzorni, Sabrina Paolino, Alberto Sulli, Vanessa Smith, Maurizio Cutolo","doi":"10.5114/reum/170845","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Glucocorticosteroids (GCs) are the most used anti-inflammatory and immunosuppressive drugs due to their effectiveness in managing pain and disease modification in many immune-inflammatory rheumatic diseases (IRDs). However, their use is limited because of adverse effects (AEs).</p><p><strong>Material and methods: </strong>The authors analyzed recent studies, including randomized controlled trials (RCTs), observational, translational studies and systematic reviews, providing an in-depth viewpoint on the benefits and drawbacks of GC use in rheumatology.</p><p><strong>Results: </strong>Glucocorticosteroids are essential in managing life-threatening autoimmune diseases and a cornerstone in many IRDs given their swift onset of action, necessary in flares. Several RCTs and meta-analyses have demonstrated that when administered over a long time and on a low-dose basis, GC can slow the radiographic progression in early rheumatoid arthritis (RA) patients by at least 50%, satisfying the conventional definition of a disease-modifying anti-rheumatic drug (DMARD). In the context of RA treatment, the use of modified-release prednisone formulations at night may offer the option of respecting circadian rhythms of both inflammatory response and HPA activation, thereby enabling low-dose GC administration to mitigate nocturnal inflammation and prolonged morning fatigue and joint stiffness. Long-term GC use should be individualized based on patient characteristics and minimized due to their potential AEs. Their chronic use, especially at medium/high dosages, might cause irreversible organ damage due to the burden of metabolic systemic effects and increased risk of infections. Many international guidelines recommend tapering/withdrawal of GCs in sustained remission. Treat-to-target (T2T) strategies are critical in setting targets for disease activity and reducing/discontinuing GCs once control is achieved.</p><p><strong>Conclusions: </strong>Glucocorticosteroids' use in treating IRDs should be judicious, focused on minimizing use, tapering and discontinuing treatment, when possible, to improve long-term safety. Glucocorticosteroids remain part of many therapeutic regimens, particularly at low doses, and elderly RA patients, especially with associated chronic comorbidities, may benefit from long-term low-dose GC treatment. A personalized GC therapy is essential for optimal long-term outcomes.</p>","PeriodicalId":21312,"journal":{"name":"Reumatologia","volume":"61 4","pages":"283-293"},"PeriodicalIF":1.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/44/17/RU-61-170845.PMC10515127.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reumatologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/reum/170845","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/31 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Glucocorticosteroids (GCs) are the most used anti-inflammatory and immunosuppressive drugs due to their effectiveness in managing pain and disease modification in many immune-inflammatory rheumatic diseases (IRDs). However, their use is limited because of adverse effects (AEs).
Material and methods: The authors analyzed recent studies, including randomized controlled trials (RCTs), observational, translational studies and systematic reviews, providing an in-depth viewpoint on the benefits and drawbacks of GC use in rheumatology.
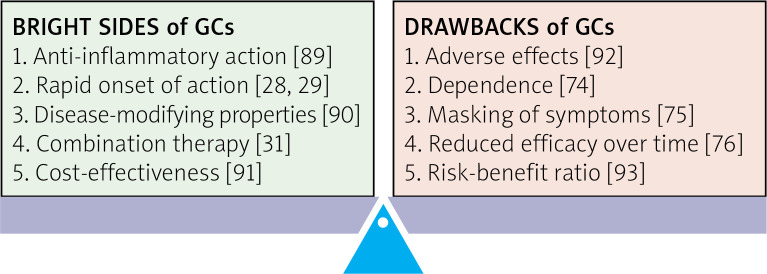
Results: Glucocorticosteroids are essential in managing life-threatening autoimmune diseases and a cornerstone in many IRDs given their swift onset of action, necessary in flares. Several RCTs and meta-analyses have demonstrated that when administered over a long time and on a low-dose basis, GC can slow the radiographic progression in early rheumatoid arthritis (RA) patients by at least 50%, satisfying the conventional definition of a disease-modifying anti-rheumatic drug (DMARD). In the context of RA treatment, the use of modified-release prednisone formulations at night may offer the option of respecting circadian rhythms of both inflammatory response and HPA activation, thereby enabling low-dose GC administration to mitigate nocturnal inflammation and prolonged morning fatigue and joint stiffness. Long-term GC use should be individualized based on patient characteristics and minimized due to their potential AEs. Their chronic use, especially at medium/high dosages, might cause irreversible organ damage due to the burden of metabolic systemic effects and increased risk of infections. Many international guidelines recommend tapering/withdrawal of GCs in sustained remission. Treat-to-target (T2T) strategies are critical in setting targets for disease activity and reducing/discontinuing GCs once control is achieved.
Conclusions: Glucocorticosteroids' use in treating IRDs should be judicious, focused on minimizing use, tapering and discontinuing treatment, when possible, to improve long-term safety. Glucocorticosteroids remain part of many therapeutic regimens, particularly at low doses, and elderly RA patients, especially with associated chronic comorbidities, may benefit from long-term low-dose GC treatment. A personalized GC therapy is essential for optimal long-term outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


