Sherry Zhang MD , Joan C. Lo MD , Marc G. Jaffe MD , Hasmik Arzumanyan MD
{"title":"Elevated Serum Androstenedione Level in a Patient With Ectopic Adrenocorticotropic Hormone Syndrome","authors":"Sherry Zhang MD , Joan C. Lo MD , Marc G. Jaffe MD , Hasmik Arzumanyan MD","doi":"10.1016/j.aace.2023.04.009","DOIUrl":null,"url":null,"abstract":"<div><h3>Background/Objective</h3><p>Ectopic Cushing syndrome can be challenging to diagnose when its presentation is atypical. Herein, we highlight features of ectopic adrenocorticotropic hormone (ACTH) syndrome in a patient with worsening hypertension, hypokalemia, ACTH-dependent hypercortisolism, and disproportionate elevation in serum androstenedione levels.</p></div><div><h3>Case Report</h3><p>A 59-year-old woman presented with rapidly progressing hypertension, severe hypokalemia, confusion, and weakness. Her medical history included well-controlled hypertension receiving amlodipine 5 mg/day, which worsened 3 months prior to admission requiring losartan and spironolactone therapy, with twice daily potassium supplementation. Physical examination was notable for bruising, muscle wasting, thin extremities, facial fullness, and abdominal adiposity despite body mass index 17 kg/m<sup>2</sup>. Laboratory evaluation showed potassium 2.6 mEq/L (3.5-5.3), morning cortisol >50 mcg/dL (8-25), 24-hour urine cortisol 8369 mcg/day (<50), ACTH 308 pg/mL (<46), androstenedione 398 ng/dL (20-75), dehydroepiandrosterone sulfate 48 mcg/dL (≤430), and testosterone 11 ng/dL (≤4.5) levels. A 3.8-cm carcinoid right lung tumor was identified, and resection was performed with clean margins. Cortisol, androstenedione, and potassium levels rapidly normalized postoperatively and blood pressure returned to baseline, well-controlled on amlodipine.</p></div><div><h3>Discussion</h3><p>Our case illustrates disproportionate elevation in androstenedione levels despite normal dehydroepiandrosterone sulfate and testosterone in a woman with ectopic ACTH syndrome. Limited reports have observed similar discordance in androgen profiles in ectopic versus pituitary ACTH hypersecretion, potentially attributable to differential activation of androgen biosynthesis.</p></div><div><h3>Conclusion</h3><p>Adrenal androgen assessment may help differentiate pituitary versus ectopic ACTH secretion in which androstenedione is elevated, but studies are needed to determine whether disproportionate androstenedione elevation reliably predicts the origin of ACTH excess.</p></div>","PeriodicalId":7051,"journal":{"name":"AACE Clinical Case Reports","volume":"9 5","pages":"Pages 142-145"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10509380/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AACE Clinical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2376060523000949","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 2
Abstract
Background/Objective
Ectopic Cushing syndrome can be challenging to diagnose when its presentation is atypical. Herein, we highlight features of ectopic adrenocorticotropic hormone (ACTH) syndrome in a patient with worsening hypertension, hypokalemia, ACTH-dependent hypercortisolism, and disproportionate elevation in serum androstenedione levels.
Case Report
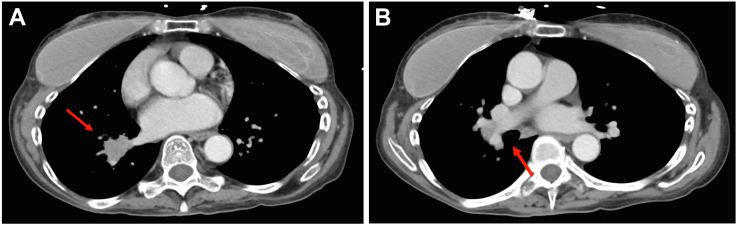
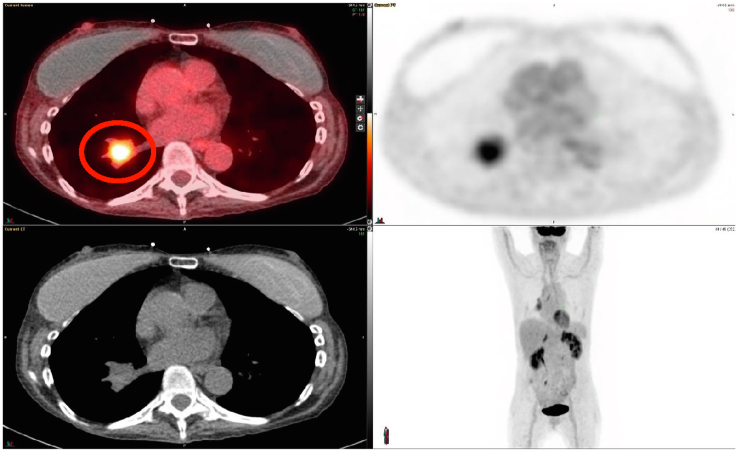
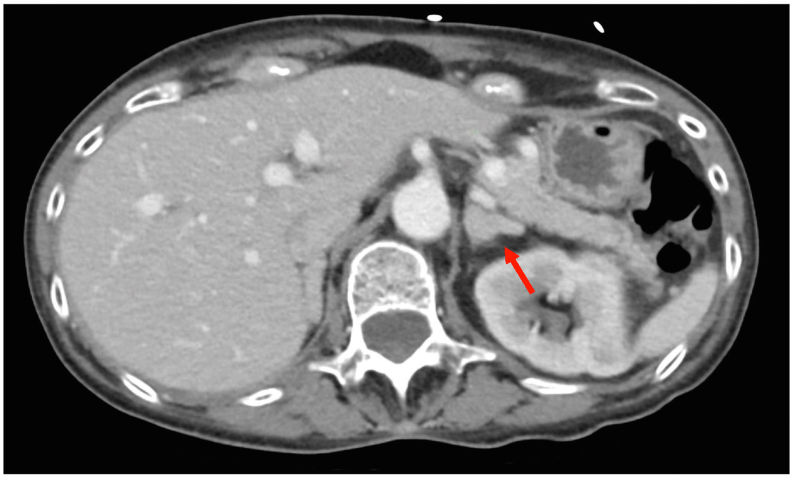
A 59-year-old woman presented with rapidly progressing hypertension, severe hypokalemia, confusion, and weakness. Her medical history included well-controlled hypertension receiving amlodipine 5 mg/day, which worsened 3 months prior to admission requiring losartan and spironolactone therapy, with twice daily potassium supplementation. Physical examination was notable for bruising, muscle wasting, thin extremities, facial fullness, and abdominal adiposity despite body mass index 17 kg/m2. Laboratory evaluation showed potassium 2.6 mEq/L (3.5-5.3), morning cortisol >50 mcg/dL (8-25), 24-hour urine cortisol 8369 mcg/day (<50), ACTH 308 pg/mL (<46), androstenedione 398 ng/dL (20-75), dehydroepiandrosterone sulfate 48 mcg/dL (≤430), and testosterone 11 ng/dL (≤4.5) levels. A 3.8-cm carcinoid right lung tumor was identified, and resection was performed with clean margins. Cortisol, androstenedione, and potassium levels rapidly normalized postoperatively and blood pressure returned to baseline, well-controlled on amlodipine.
Discussion
Our case illustrates disproportionate elevation in androstenedione levels despite normal dehydroepiandrosterone sulfate and testosterone in a woman with ectopic ACTH syndrome. Limited reports have observed similar discordance in androgen profiles in ectopic versus pituitary ACTH hypersecretion, potentially attributable to differential activation of androgen biosynthesis.
Conclusion
Adrenal androgen assessment may help differentiate pituitary versus ectopic ACTH secretion in which androstenedione is elevated, but studies are needed to determine whether disproportionate androstenedione elevation reliably predicts the origin of ACTH excess.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


