Kenichiro Suyama, Shoji Matsumoto, Ichiro Nakahara, Yoshio Suyama, Jun Morioka, Akiko Hasebe, Jun Tanabe, Sadayoshi Watanabe, Kiyonori Kuwahara, Yuichi Hirose
{"title":"Delays in initial workflow cause delayed initiation of mechanical thrombectomy in patients with in-hospital ischemic stroke.","authors":"Kenichiro Suyama, Shoji Matsumoto, Ichiro Nakahara, Yoshio Suyama, Jun Morioka, Akiko Hasebe, Jun Tanabe, Sadayoshi Watanabe, Kiyonori Kuwahara, Yuichi Hirose","doi":"10.20407/fmj.2021-014","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The benefit of mechanical thrombectomy for acute ischemic stroke is highly time dependent. However, time to treatment is longer for in-hospital stroke patients than community-onset stroke patients. This study aimed to clarify the cause of this difference.</p><p><strong>Methods: </strong>A retrospective single-center study was performed to analyze patients with large vessel occlusion who underwent mechanical thrombectomy between January 2017 and December 2019. Patients were divided into in-hospital stroke and community-onset stroke groups. Clinical characteristics and treatment time intervals were compared between groups.</p><p><strong>Results: </strong>One hundred four patients were analyzed: 17 with in-hospital stroke and 87 with community-onset stroke. Patient characteristics did not significantly differ between groups. Median door (stroke recognition)-to-computed tomography time (36 min vs. 14 min, P<0.01) and door-to-puncture time (135 min vs. 117 min, P=0.02) were significantly longer in the in-hospital stroke group than the community-onset stroke group. However, median computed tomography-to-puncture time (104 min vs. 104 min, P=0.47) and puncture-to-reperfusion time (53 min vs. 38 min, P=0.17) did not significantly differ.</p><p><strong>Conclusions: </strong>Longer door-to-puncture time in in-hospital stroke patients was mostly caused by longer door-to-computed tomography time, which is the initial part of the workflow. An in-hospital stroke protocol that places importance on early stroke specialist consultation and prompt transportation to the computed tomography scanner might hasten treatment and improve outcomes in patients with in-hospital stroke.</p>","PeriodicalId":33657,"journal":{"name":"Fujita Medical Journal","volume":"8 3","pages":"73-78"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9358672/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Fujita Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20407/fmj.2021-014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/11/25 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Objectives: The benefit of mechanical thrombectomy for acute ischemic stroke is highly time dependent. However, time to treatment is longer for in-hospital stroke patients than community-onset stroke patients. This study aimed to clarify the cause of this difference.
Methods: A retrospective single-center study was performed to analyze patients with large vessel occlusion who underwent mechanical thrombectomy between January 2017 and December 2019. Patients were divided into in-hospital stroke and community-onset stroke groups. Clinical characteristics and treatment time intervals were compared between groups.
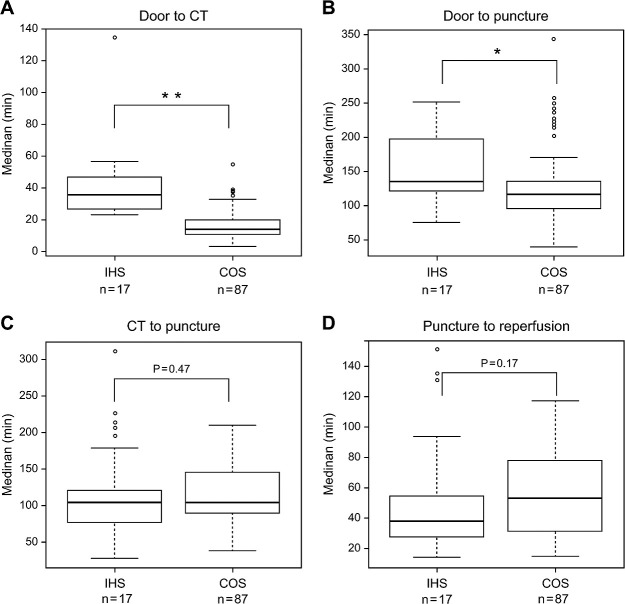
Results: One hundred four patients were analyzed: 17 with in-hospital stroke and 87 with community-onset stroke. Patient characteristics did not significantly differ between groups. Median door (stroke recognition)-to-computed tomography time (36 min vs. 14 min, P<0.01) and door-to-puncture time (135 min vs. 117 min, P=0.02) were significantly longer in the in-hospital stroke group than the community-onset stroke group. However, median computed tomography-to-puncture time (104 min vs. 104 min, P=0.47) and puncture-to-reperfusion time (53 min vs. 38 min, P=0.17) did not significantly differ.
Conclusions: Longer door-to-puncture time in in-hospital stroke patients was mostly caused by longer door-to-computed tomography time, which is the initial part of the workflow. An in-hospital stroke protocol that places importance on early stroke specialist consultation and prompt transportation to the computed tomography scanner might hasten treatment and improve outcomes in patients with in-hospital stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


