Gabriel Sjölin, Torquil Watt, Kristina Byström, Jan Calissendorff, Per Karkov Cramon, Helena Filipsson Nyström, Bengt Hallengren, Mats Holmberg, Selwan Khamisi, Mikael Lantz, Tereza Planck, Ove Törring, Göran Wallin
{"title":"Long term outcome after toxic nodular goitre.","authors":"Gabriel Sjölin, Torquil Watt, Kristina Byström, Jan Calissendorff, Per Karkov Cramon, Helena Filipsson Nyström, Bengt Hallengren, Mats Holmberg, Selwan Khamisi, Mikael Lantz, Tereza Planck, Ove Törring, Göran Wallin","doi":"10.1186/s13044-022-00138-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The purpose of treating toxic nodular goitre (TNG) is to reverse hyperthyroidism, prevent recurrent disease, relieve symptoms and preserve thyroid function. Treatment efficacies and long-term outcomes of antithyroid drugs (ATD), radioactive iodine (RAI) or surgery vary in the literature. Symptoms often persist for a long time following euthyroidism, and previous studies have demonstrated long-term cognitive and quality of life (QoL) impairments. We report the outcome of treatment, rate of cure (euthyroidism and hypothyroidism), and QoL in an unselected TNG cohort.</p><p><strong>Methods: </strong>TNG patients (n = 638) de novo diagnosed between 2003-2005 were invited to engage in a 6-10-year follow-up study. 237 patients responded to questionnaires about therapies, demographics, comorbidities, and quality of life (ThyPRO). Patients received ATD, RAI, or surgery according clinical guidelines.</p><p><strong>Results: </strong>The fraction of patients cured with one RAI treatment was 89%, and 93% in patients treated with surgery. The rate of levothyroxine supplementation for RAI and surgery, at the end of the study period, was 58% respectively 64%. Approximately 5% of the patients needed three or more RAI treatments to be cured. The patients had worse thyroid-related QoL scores, in a broad spectrum, than the general population.</p><p><strong>Conclusion: </strong>One advantage of treating TNG with RAI over surgery might be lost due to the seemingly similar incidence of hypothyroidism. The need for up to five treatments is rarely described and indicates that the treatment of TNG can be more complex than expected. This circumstance and the long-term QoL impairments are reminders of the chronic nature of hyperthyroidism from TNG.</p>","PeriodicalId":39048,"journal":{"name":"Thyroid Research","volume":" ","pages":"20"},"PeriodicalIF":1.8000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9624053/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thyroid Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13044-022-00138-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The purpose of treating toxic nodular goitre (TNG) is to reverse hyperthyroidism, prevent recurrent disease, relieve symptoms and preserve thyroid function. Treatment efficacies and long-term outcomes of antithyroid drugs (ATD), radioactive iodine (RAI) or surgery vary in the literature. Symptoms often persist for a long time following euthyroidism, and previous studies have demonstrated long-term cognitive and quality of life (QoL) impairments. We report the outcome of treatment, rate of cure (euthyroidism and hypothyroidism), and QoL in an unselected TNG cohort.
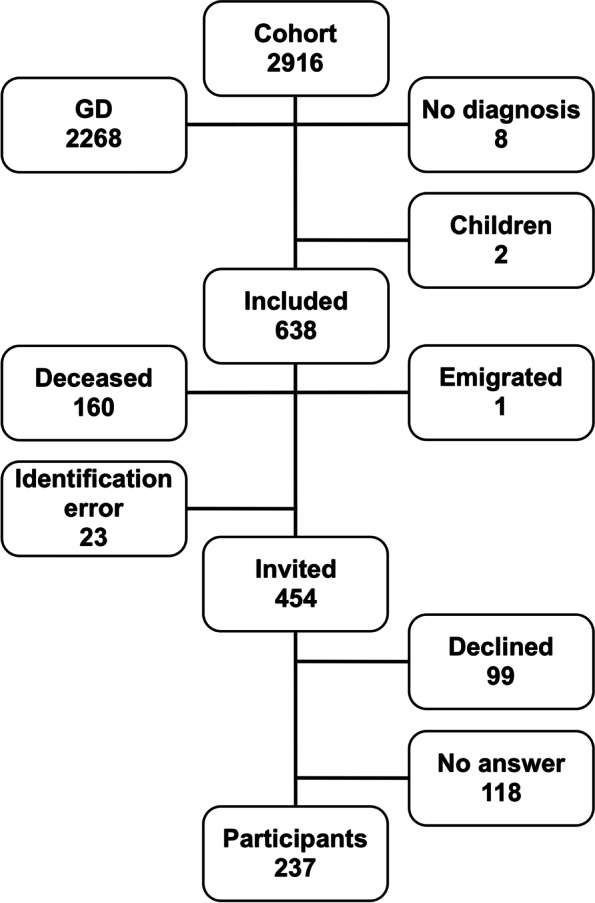
Methods: TNG patients (n = 638) de novo diagnosed between 2003-2005 were invited to engage in a 6-10-year follow-up study. 237 patients responded to questionnaires about therapies, demographics, comorbidities, and quality of life (ThyPRO). Patients received ATD, RAI, or surgery according clinical guidelines.
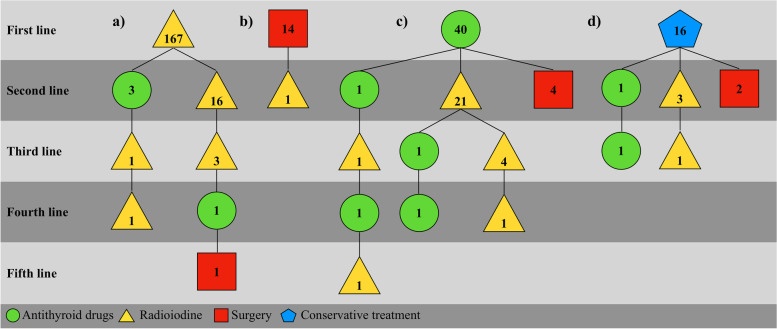
Results: The fraction of patients cured with one RAI treatment was 89%, and 93% in patients treated with surgery. The rate of levothyroxine supplementation for RAI and surgery, at the end of the study period, was 58% respectively 64%. Approximately 5% of the patients needed three or more RAI treatments to be cured. The patients had worse thyroid-related QoL scores, in a broad spectrum, than the general population.
Conclusion: One advantage of treating TNG with RAI over surgery might be lost due to the seemingly similar incidence of hypothyroidism. The need for up to five treatments is rarely described and indicates that the treatment of TNG can be more complex than expected. This circumstance and the long-term QoL impairments are reminders of the chronic nature of hyperthyroidism from TNG.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


