Leif Simmatis, Carolina Barnett, Reeman Marzouqah, Babak Taati, Mark Boulos, Yana Yunusova
{"title":"Reliability of Automatic Computer Vision-Based Assessment of Orofacial Kinematics for Telehealth Applications.","authors":"Leif Simmatis, Carolina Barnett, Reeman Marzouqah, Babak Taati, Mark Boulos, Yana Yunusova","doi":"10.1159/000525698","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Telehealth/remote assessment using readily available 2D mobile cameras and deep learning-based analyses is rapidly becoming a viable option for detecting orofacial and speech impairments associated with neurological and neurodegenerative disease during telehealth practice. However, the psychometric properties (e.g., internal consistency and reliability) of kinematics obtained from these systems have not been established, which is a crucial next step before their clinical usability is established.</p><p><strong>Methods: </strong>Participants were assessed in lab using a 3 dimensional (3D)-capable camera and at home using a readily-available 2D camera in a tablet. Orofacial kinematics was estimated from videos using a deep facial landmark tracking model. Kinematic features quantified the clinically relevant constructs of velocity, range of motion, and lateralization. In lab, all participants performed the same oromotor task. At home, participants were split into two groups that each performed a variant of the in-lab task. We quantified within-assessment consistency (Cronbach's α), reliability (intraclass correlation coefficient [ICC]), and fitted linear mixed-effects models to at-home data to capture individual-/task-dependent longitudinal trajectories.</p><p><strong>Results: </strong>Both in lab and at home, Cronbach's α was typically high (>0.80) and ICCs were often good (>0.70). The linear mixed-effect models that best fit the longitudinal data were those that accounted for individual- or task-dependent effects.</p><p><strong>Discussion: </strong>Remotely gathered orofacial kinematics were as internally consistent and reliable as those gathered in a controlled laboratory setting using a high-performance 3D-capable camera and could additionally capture individual- or task-dependent changes over time. These results highlight the potential of remote assessment tools as digital biomarkers of disease status and progression and demonstrate their suitability for novel telehealth applications.</p>","PeriodicalId":11242,"journal":{"name":"Digital Biomarkers","volume":"6 2","pages":"71-82"},"PeriodicalIF":0.0000,"publicationDate":"2022-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c1/96/dib-0006-0071.PMC9574208.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digital Biomarkers","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000525698","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Computer Science","Score":null,"Total":0}
引用次数: 2
Abstract
Introduction: Telehealth/remote assessment using readily available 2D mobile cameras and deep learning-based analyses is rapidly becoming a viable option for detecting orofacial and speech impairments associated with neurological and neurodegenerative disease during telehealth practice. However, the psychometric properties (e.g., internal consistency and reliability) of kinematics obtained from these systems have not been established, which is a crucial next step before their clinical usability is established.
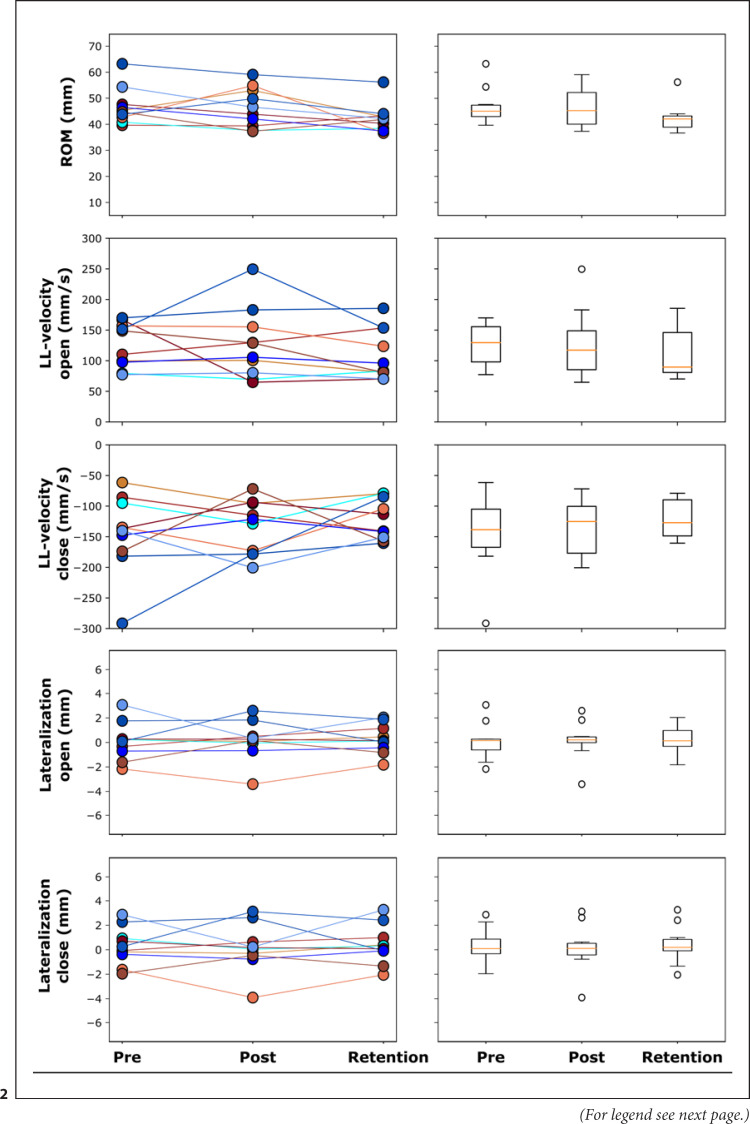
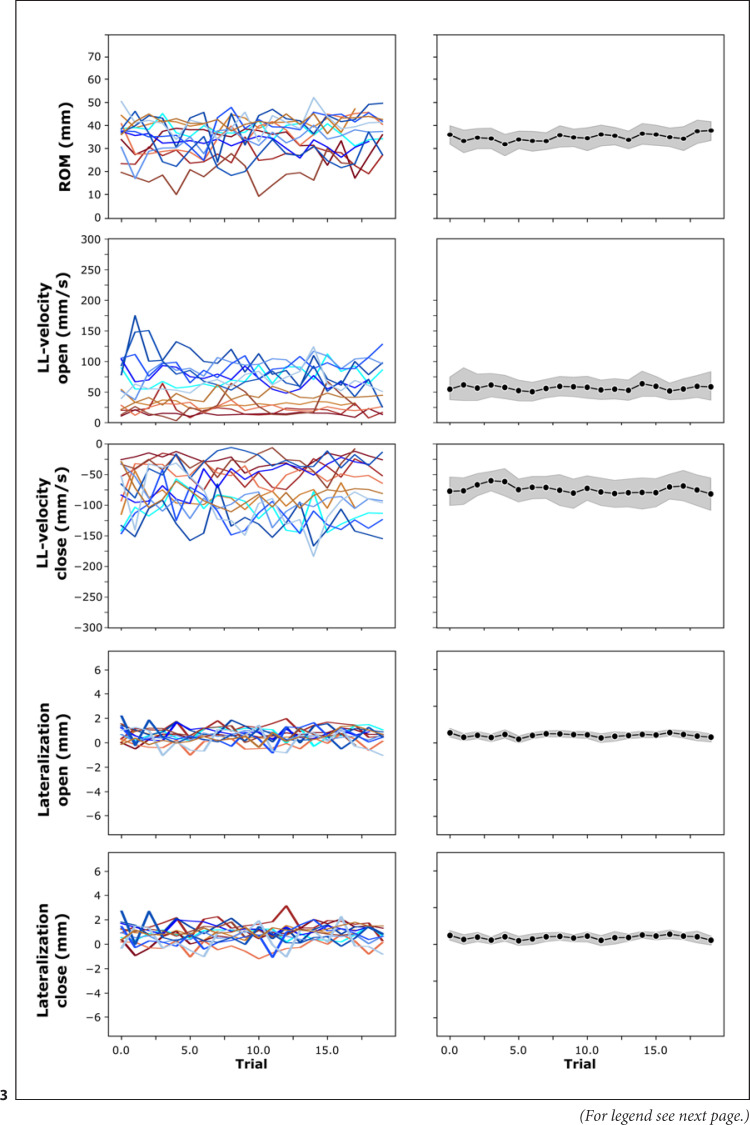
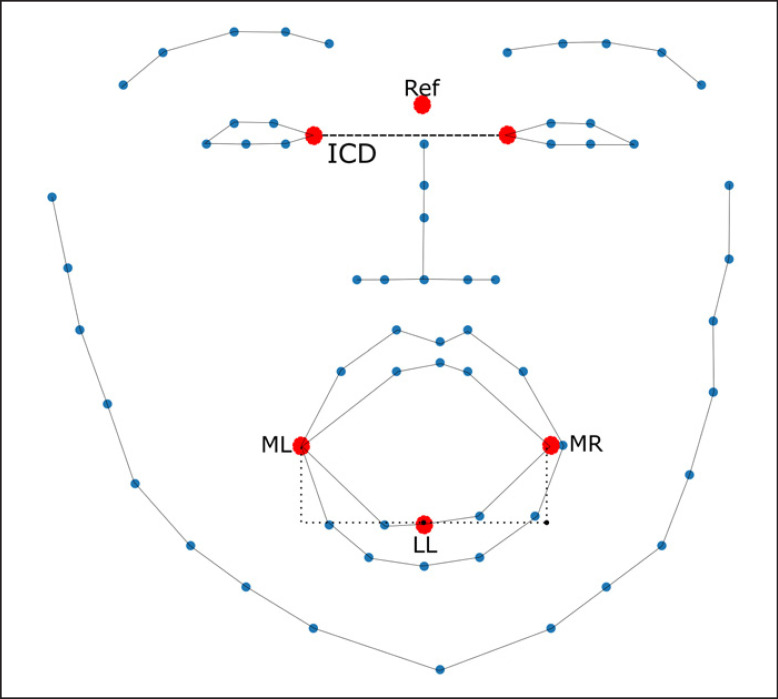
Methods: Participants were assessed in lab using a 3 dimensional (3D)-capable camera and at home using a readily-available 2D camera in a tablet. Orofacial kinematics was estimated from videos using a deep facial landmark tracking model. Kinematic features quantified the clinically relevant constructs of velocity, range of motion, and lateralization. In lab, all participants performed the same oromotor task. At home, participants were split into two groups that each performed a variant of the in-lab task. We quantified within-assessment consistency (Cronbach's α), reliability (intraclass correlation coefficient [ICC]), and fitted linear mixed-effects models to at-home data to capture individual-/task-dependent longitudinal trajectories.
Results: Both in lab and at home, Cronbach's α was typically high (>0.80) and ICCs were often good (>0.70). The linear mixed-effect models that best fit the longitudinal data were those that accounted for individual- or task-dependent effects.
Discussion: Remotely gathered orofacial kinematics were as internally consistent and reliable as those gathered in a controlled laboratory setting using a high-performance 3D-capable camera and could additionally capture individual- or task-dependent changes over time. These results highlight the potential of remote assessment tools as digital biomarkers of disease status and progression and demonstrate their suitability for novel telehealth applications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


