Robert R Ehrman, Bryce X Bredell, Nicholas E Harrison, Mark J Favot, Brian D Haber, Robert D Welch, Philip D Levy, Robert L Sherwin
{"title":"Increasing illness severity is associated with global myocardial dysfunction in the first 24 hours of sepsis admission.","authors":"Robert R Ehrman, Bryce X Bredell, Nicholas E Harrison, Mark J Favot, Brian D Haber, Robert D Welch, Philip D Levy, Robert L Sherwin","doi":"10.1186/s13089-022-00282-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Septic cardiomyopathy was recognized more than 30 years ago, but the early phase remains uncharacterized as no existing studies captured patients at the time of Emergency Department (ED) presentation, prior to resuscitation. Therapeutic interventions alter cardiac function, thereby distorting the relationship with disease severity and outcomes. The goal of this study was to assess the impact of illness severity on cardiac function during the first 24 h of sepsis admission.</p><p><strong>Methods: </strong>This was a pre-planned secondary analysis of a prospective observational study of adults presenting to the ED with suspected sepsis (treatment for infection plus either lactate > 2 mmol/liter or systolic blood pressure < 90 mm/Hg) who received < 1L IV fluid before enrollment. Patients had 3 echocardiograms performed (presentation, 3, and 24 h). The primary outcome was the effect of increasing sepsis illness severity, defined by ED Sequential Organ Failure Assessment (SOFA) score, on parameters of cardiac function, assessed using linear mixed-effects models. The secondary goal was to determine whether cardiac function differed between survivors and non-survivors, also using mixed-effects models.</p><p><strong>Results: </strong>We enrolled 73 patients with a mean age of 60 (SD 16.1) years and in-hospital mortality of 23%. For the primary analysis, we found that increasing ED SOFA score was associated with worse cardiac function over the first 24 h across all assessed parameters of left-ventricular systolic and diastolic function as well as right-ventricular systolic function. While baseline strain and E/e' were better in survivors, in the mixed models analysis, the trajectory of Global Longitudinal Strain and septal E/e' over the first 24 h of illness differed between survivors and non-survivors, with improved function at 24 h in non-survivors.</p><p><strong>Conclusions: </strong>In the first study to capture patients prior to the initiation of resuscitation, we found a direct relationship between sepsis severity and global myocardial dysfunction. Future studies are needed to confirm these results, to identify myocardial depressants, and to investigate the link with adverse outcomes so that therapeutic interventions can be developed.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":" ","pages":"32"},"PeriodicalIF":3.4000,"publicationDate":"2022-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9334514/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-022-00282-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Septic cardiomyopathy was recognized more than 30 years ago, but the early phase remains uncharacterized as no existing studies captured patients at the time of Emergency Department (ED) presentation, prior to resuscitation. Therapeutic interventions alter cardiac function, thereby distorting the relationship with disease severity and outcomes. The goal of this study was to assess the impact of illness severity on cardiac function during the first 24 h of sepsis admission.
Methods: This was a pre-planned secondary analysis of a prospective observational study of adults presenting to the ED with suspected sepsis (treatment for infection plus either lactate > 2 mmol/liter or systolic blood pressure < 90 mm/Hg) who received < 1L IV fluid before enrollment. Patients had 3 echocardiograms performed (presentation, 3, and 24 h). The primary outcome was the effect of increasing sepsis illness severity, defined by ED Sequential Organ Failure Assessment (SOFA) score, on parameters of cardiac function, assessed using linear mixed-effects models. The secondary goal was to determine whether cardiac function differed between survivors and non-survivors, also using mixed-effects models.
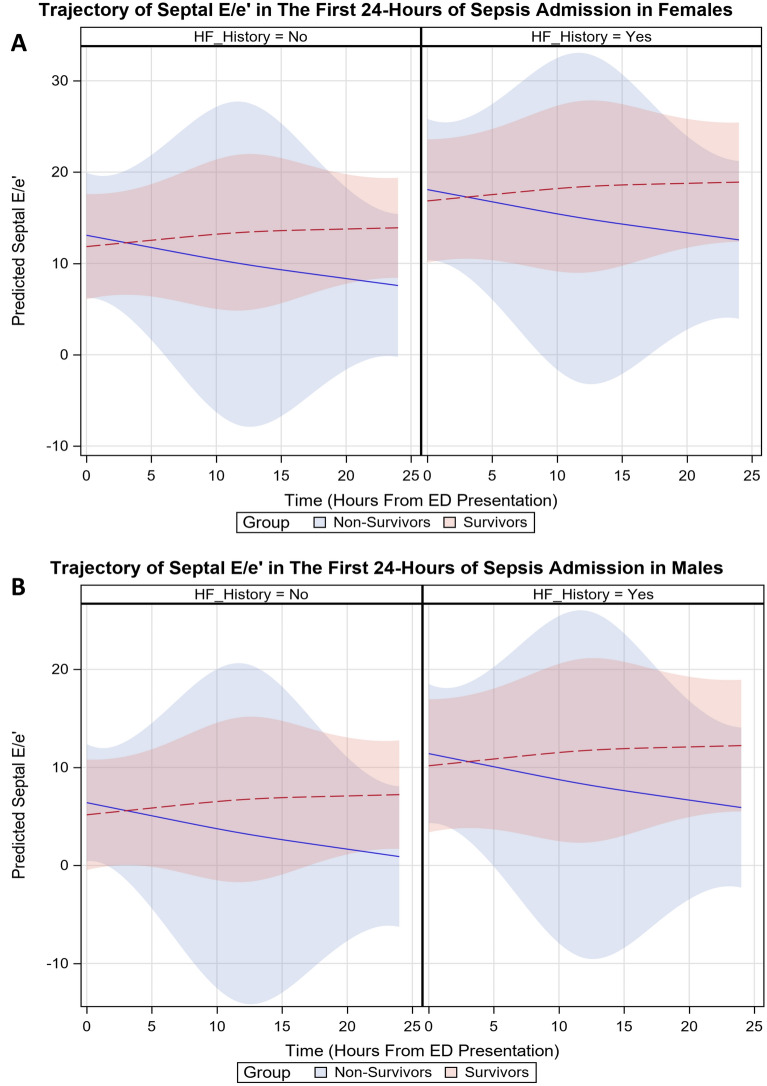
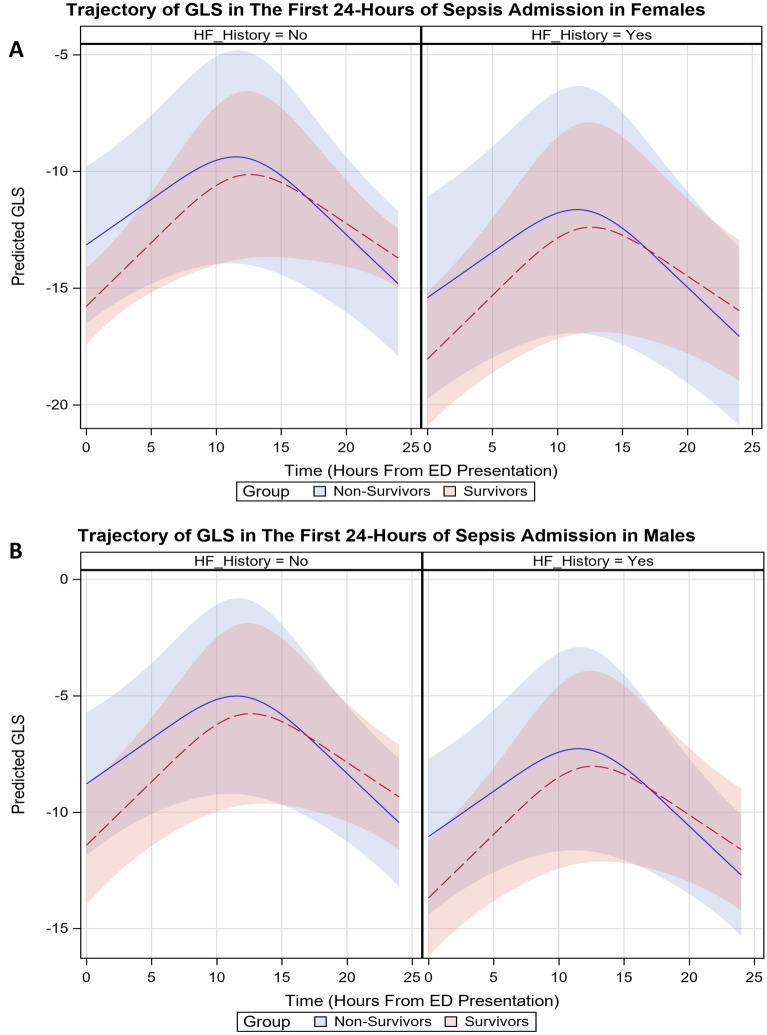
Results: We enrolled 73 patients with a mean age of 60 (SD 16.1) years and in-hospital mortality of 23%. For the primary analysis, we found that increasing ED SOFA score was associated with worse cardiac function over the first 24 h across all assessed parameters of left-ventricular systolic and diastolic function as well as right-ventricular systolic function. While baseline strain and E/e' were better in survivors, in the mixed models analysis, the trajectory of Global Longitudinal Strain and septal E/e' over the first 24 h of illness differed between survivors and non-survivors, with improved function at 24 h in non-survivors.
Conclusions: In the first study to capture patients prior to the initiation of resuscitation, we found a direct relationship between sepsis severity and global myocardial dysfunction. Future studies are needed to confirm these results, to identify myocardial depressants, and to investigate the link with adverse outcomes so that therapeutic interventions can be developed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


