{"title":"Effectiveness of the Use of Standardized Vocabularies on Epilepsy Patient Cohort Generation.","authors":"Hyesil Jung, Ho-Young Lee, Sooyoung Yoo, Hee Hwang, Hyunyoung Baek","doi":"10.4258/hir.2022.28.3.240","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This study investigated the effectiveness of using standardized vocabularies to generate epilepsy patient cohorts with local medical codes, SNOMED Clinical Terms (SNOMED CT), and International Classification of Diseases tenth revision (ICD-10)/Korean Classification of Diseases-7 (KCD-7).</p><p><strong>Methods: </strong>We compared the granularity between SNOMED CT and ICD-10 for epilepsy by counting the number of SNOMED CT concepts mapped to one ICD-10 code. Next, we created epilepsy patient cohorts by selecting all patients who had at least one code included in the concept sets defined using each vocabulary. We set patient cohorts generated by local codes as the reference to evaluate the patient cohorts generated using SNOMED CT and ICD-10/KCD-7. We compared the number of patients, the prevalence of epilepsy, and the age distribution between patient cohorts by year.</p><p><strong>Results: </strong>In terms of the cohort size, the match rate with the reference cohort was approximately 99.2% for SNOMED CT and 94.0% for ICD-10/KDC7. From 2010 to 2019, the mean prevalence of epilepsy defined using the local codes, SNOMED CT, and ICD-10/KCD-7 was 0.889%, 0.891% and 0.923%, respectively. The age distribution of epilepsy patients showed no significant difference between the cohorts defined using local codes or SNOMED CT, but the ICD-9/KCD-7-generated cohort showed a substantial gap in the age distribution of patients with epilepsy compared to the cohort generated using the local codes.</p><p><strong>Conclusions: </strong>The number and age distribution of patients were substantially different from the reference when we used ICD-10/KCD-7 codes, but not when we used SNOMED CT concepts. Therefore, SNOMED CT is more suitable for representing clinical ideas and conducting clinical studies than ICD-10/KCD-7.</p>","PeriodicalId":2,"journal":{"name":"ACS Applied Bio Materials","volume":" ","pages":"240-246"},"PeriodicalIF":4.6000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/65/c6/hir-2022-28-3-240.PMC9388923.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Bio Materials","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4258/hir.2022.28.3.240","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/31 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MATERIALS SCIENCE, BIOMATERIALS","Score":null,"Total":0}
引用次数: 1
Abstract
Objectives: This study investigated the effectiveness of using standardized vocabularies to generate epilepsy patient cohorts with local medical codes, SNOMED Clinical Terms (SNOMED CT), and International Classification of Diseases tenth revision (ICD-10)/Korean Classification of Diseases-7 (KCD-7).
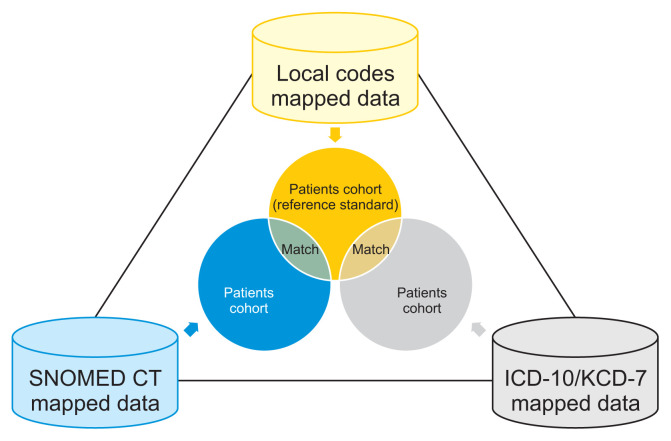
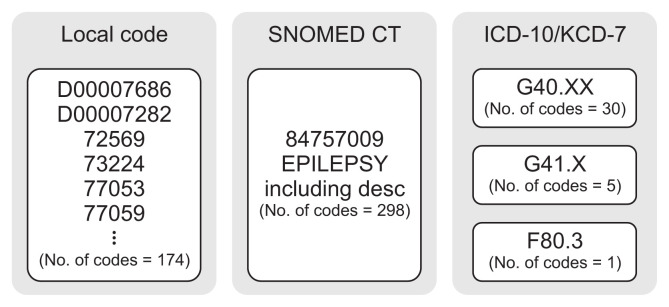
Methods: We compared the granularity between SNOMED CT and ICD-10 for epilepsy by counting the number of SNOMED CT concepts mapped to one ICD-10 code. Next, we created epilepsy patient cohorts by selecting all patients who had at least one code included in the concept sets defined using each vocabulary. We set patient cohorts generated by local codes as the reference to evaluate the patient cohorts generated using SNOMED CT and ICD-10/KCD-7. We compared the number of patients, the prevalence of epilepsy, and the age distribution between patient cohorts by year.
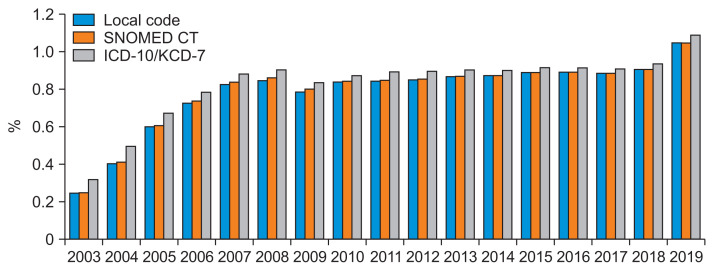
Results: In terms of the cohort size, the match rate with the reference cohort was approximately 99.2% for SNOMED CT and 94.0% for ICD-10/KDC7. From 2010 to 2019, the mean prevalence of epilepsy defined using the local codes, SNOMED CT, and ICD-10/KCD-7 was 0.889%, 0.891% and 0.923%, respectively. The age distribution of epilepsy patients showed no significant difference between the cohorts defined using local codes or SNOMED CT, but the ICD-9/KCD-7-generated cohort showed a substantial gap in the age distribution of patients with epilepsy compared to the cohort generated using the local codes.
Conclusions: The number and age distribution of patients were substantially different from the reference when we used ICD-10/KCD-7 codes, but not when we used SNOMED CT concepts. Therefore, SNOMED CT is more suitable for representing clinical ideas and conducting clinical studies than ICD-10/KCD-7.
期刊介绍:
ACS Applied Bio Materials is an interdisciplinary journal publishing original research covering all aspects of biomaterials and biointerfaces including and beyond the traditional biosensing, biomedical and therapeutic applications.
The journal is devoted to reports of new and original experimental and theoretical research of an applied nature that integrates knowledge in the areas of materials, engineering, physics, bioscience, and chemistry into important bio applications. The journal is specifically interested in work that addresses the relationship between structure and function and assesses the stability and degradation of materials under relevant environmental and biological conditions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


