Clément Javaux, Clémentine Daveau, Clotilde Bettinger, Mathieu Daurade, Céline Dupieux-Chabert, Fabien Craighero, Carine Fuchsmann, Philippe Céruse, Arnaud Gleizal, Nicolas Sigaux, Tristan Ferry, Florent Valour, The Lyon Bji Study Group
{"title":"Osteocutaneous-flap-related osteomyelitis following mandibular reconstruction: a cohort study of an emerging and complex bone infection.","authors":"Clément Javaux, Clémentine Daveau, Clotilde Bettinger, Mathieu Daurade, Céline Dupieux-Chabert, Fabien Craighero, Carine Fuchsmann, Philippe Céruse, Arnaud Gleizal, Nicolas Sigaux, Tristan Ferry, Florent Valour, The Lyon Bji Study Group","doi":"10.5194/jbji-7-127-2022","DOIUrl":null,"url":null,"abstract":"<p><p>Osteocutaneous flap (OCF) mandible reconstruction is at high risk for surgical site infection. This study aimed to describe diagnosis, management, and outcome of OCF-related osteomyelitis. All patients managed at our institution for an OCF-related osteomyelitis following mandible reconstruction were included in a retrospective cohort study (2012-2019). Microbiology was described according to gold-standard surgical samples, considering all virulent pathogens, and potential contaminants if present on at least two samples. Determinants of treatment failure were assessed by logistic regression and Kaplan-Meier curve analysis. The 48 included patients (median age 60.5 (IQR, 52.4-66.6) years) benefited from OCF mandible reconstruction mostly for carcinoma ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>27</mn> <mo>/</mo> <mn>48</mn></mrow> </math> ; 56.3 %) or osteoradionecrosis ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>12</mn> <mo>/</mo> <mn>48</mn></mrow> </math> ; 25.0 %). OCF-related osteomyelitis was mostly early ( <math><mrow><mo>≤</mo> <mn>3</mn></mrow> </math> months post-surgery; <math><mrow><mi>n</mi> <mo>=</mo> <mn>43</mn> <mo>/</mo> <mn>48</mn></mrow> </math> ; 89.6 %), presenting with local inflammation ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>28</mn> <mo>/</mo> <mn>47</mn></mrow> </math> ; 59.6 %), nonunion (wound dehiscence) or sinus tract ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>28</mn> <mo>/</mo> <mn>47</mn></mrow> </math> ; 59.6 %), and/or bone or device exposure ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>21</mn> <mo>/</mo> <mn>47</mn></mrow> </math> ; 44.7 %). Main implicated pathogens were Enterobacteriaceae ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>25</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 61.0 %), streptococci ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>22</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 53.7 %), <i>Staphylococcus aureus</i> ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>10</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 24.4 %), enterococci ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>9</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 22.0 %), non-fermenting Gram-negative bacilli ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>8</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 19.5 %), and anaerobes ( <math><mrow><mi>n</mi> <mo>=</mo> <mn>8</mn> <mo>/</mo> <mn>41</mn></mrow> </math> ; 19.5 %). Thirty-nine patients (81.3 %) benefited from surgery, consisting of debridement with implant retention (DAIR) in <math><mrow><mn>25</mn> <mo>/</mo> <mn>39</mn></mrow> </math> (64.1 %) cases, associated with 93 (IQR, 64-128) days of antimicrobial therapy. After a follow-up of 18 (IQR, 11-31) months, <math><mrow><mn>24</mn> <mo>/</mo> <mn>48</mn></mrow> </math> (50.0 %) treatment failures were observed. Determinants of treatment outcomes were DAIR (OR, 3.333; 95 % CI, 1.020-10.898) and an early infectious disease specialist referral (OR, 0.236 if <math><mrow><mo>≤</mo> <mn>2</mn></mrow> </math> weeks; 95 % CI, 0.062-0.933). OCF-related osteomyelitis following mandibular reconstruction represents difficult-to-treat infections. Our results advocate for a multidisciplinary management, including an early infectious-disease-specialist referral to manage the antimicrobial therapy driven by complex microbiological documentation.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":" ","pages":"127-136"},"PeriodicalIF":2.8000,"publicationDate":"2022-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9285487/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-7-127-2022","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
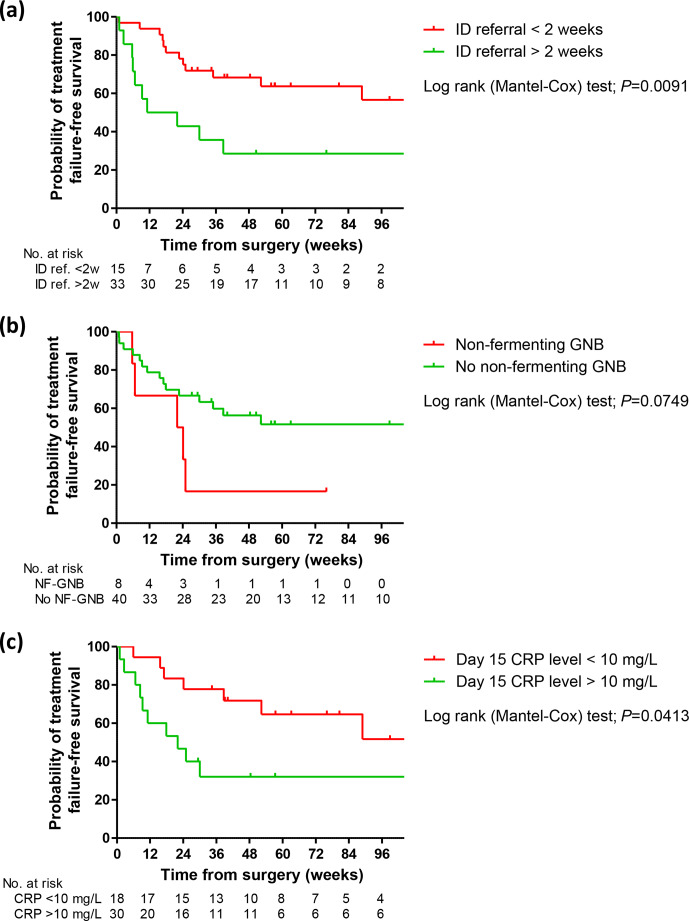
Osteocutaneous flap (OCF) mandible reconstruction is at high risk for surgical site infection. This study aimed to describe diagnosis, management, and outcome of OCF-related osteomyelitis. All patients managed at our institution for an OCF-related osteomyelitis following mandible reconstruction were included in a retrospective cohort study (2012-2019). Microbiology was described according to gold-standard surgical samples, considering all virulent pathogens, and potential contaminants if present on at least two samples. Determinants of treatment failure were assessed by logistic regression and Kaplan-Meier curve analysis. The 48 included patients (median age 60.5 (IQR, 52.4-66.6) years) benefited from OCF mandible reconstruction mostly for carcinoma ( ; 56.3 %) or osteoradionecrosis ( ; 25.0 %). OCF-related osteomyelitis was mostly early ( months post-surgery; ; 89.6 %), presenting with local inflammation ( ; 59.6 %), nonunion (wound dehiscence) or sinus tract ( ; 59.6 %), and/or bone or device exposure ( ; 44.7 %). Main implicated pathogens were Enterobacteriaceae ( ; 61.0 %), streptococci ( ; 53.7 %), Staphylococcus aureus ( ; 24.4 %), enterococci ( ; 22.0 %), non-fermenting Gram-negative bacilli ( ; 19.5 %), and anaerobes ( ; 19.5 %). Thirty-nine patients (81.3 %) benefited from surgery, consisting of debridement with implant retention (DAIR) in (64.1 %) cases, associated with 93 (IQR, 64-128) days of antimicrobial therapy. After a follow-up of 18 (IQR, 11-31) months, (50.0 %) treatment failures were observed. Determinants of treatment outcomes were DAIR (OR, 3.333; 95 % CI, 1.020-10.898) and an early infectious disease specialist referral (OR, 0.236 if weeks; 95 % CI, 0.062-0.933). OCF-related osteomyelitis following mandibular reconstruction represents difficult-to-treat infections. Our results advocate for a multidisciplinary management, including an early infectious-disease-specialist referral to manage the antimicrobial therapy driven by complex microbiological documentation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


