Postoperative Complications and Their Risk Factors of Completion Total Gastrectomy for Remnant Gastric Cancer Following an Initial Gastrectomy for Cancer.
Sin Hye Park, Sang Soo Eom, Bang Wool Eom, Hong Man Yoon, Young-Woo Kim, Keun Won Ryu
{"title":"Postoperative Complications and Their Risk Factors of Completion Total Gastrectomy for Remnant Gastric Cancer Following an Initial Gastrectomy for Cancer.","authors":"Sin Hye Park, Sang Soo Eom, Bang Wool Eom, Hong Man Yoon, Young-Woo Kim, Keun Won Ryu","doi":"10.5230/jgc.2022.22.e19","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Completion total gastrectomy (CTG) for remnant gastric cancer (RGC) is a technically demanding procedure and associated with increased morbidity. The present study aimed to evaluate postoperative complications and their risk factors following surgery for RGC after initial partial gastrectomy due to gastric cancer excluding peptic ulcer.</p><p><strong>Materials and methods: </strong>We retrospectively reviewed the data of 107 patients who had previously undergone an initial gastric cancer surgery and subsequently underwent CTG for RGC between March 2002 and December 2020. The postoperative complications were graded using the Clavien-Dindo classification. Logistic regression analyses were used to determine the risk factors for complications.</p><p><strong>Results: </strong>Postoperative complications occurred in 34.6% (37/107) of the patients. Intra-abdominal abscess was the most common complication. The significant risk factors for overall complications were multi-visceral resections, longer operation time, and high estimated blood loss in the univariate analysis. The independent risk factors were multi-visceral resection (odds ratio [OR], 2.832; 95% confidence interval [CI], 1.094-7.333; P=0.032) and longer operation time (OR, 1.005; 95% CI, 1.001-1.011; P=0.036) in the multivariate analysis. Previous reconstruction type, minimally invasive approach, and current stage were not associated with the overall complications.</p><p><strong>Conclusions: </strong>Multi-visceral resection and long operation time were significant risk factors for the occurrence of complications following CTG rather than the RGC stage or surgical approach. When multi-visceral resection is required, a more meticulous surgical procedure is warranted to improve the postoperative complications during CTG for RGC after an initial gastric cancer surgery.</p>","PeriodicalId":56072,"journal":{"name":"Journal of Gastric Cancer","volume":"22 3","pages":"210-219"},"PeriodicalIF":3.2000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0e/42/jgc-22-210.PMC9359885.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastric Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5230/jgc.2022.22.e19","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Purpose: Completion total gastrectomy (CTG) for remnant gastric cancer (RGC) is a technically demanding procedure and associated with increased morbidity. The present study aimed to evaluate postoperative complications and their risk factors following surgery for RGC after initial partial gastrectomy due to gastric cancer excluding peptic ulcer.
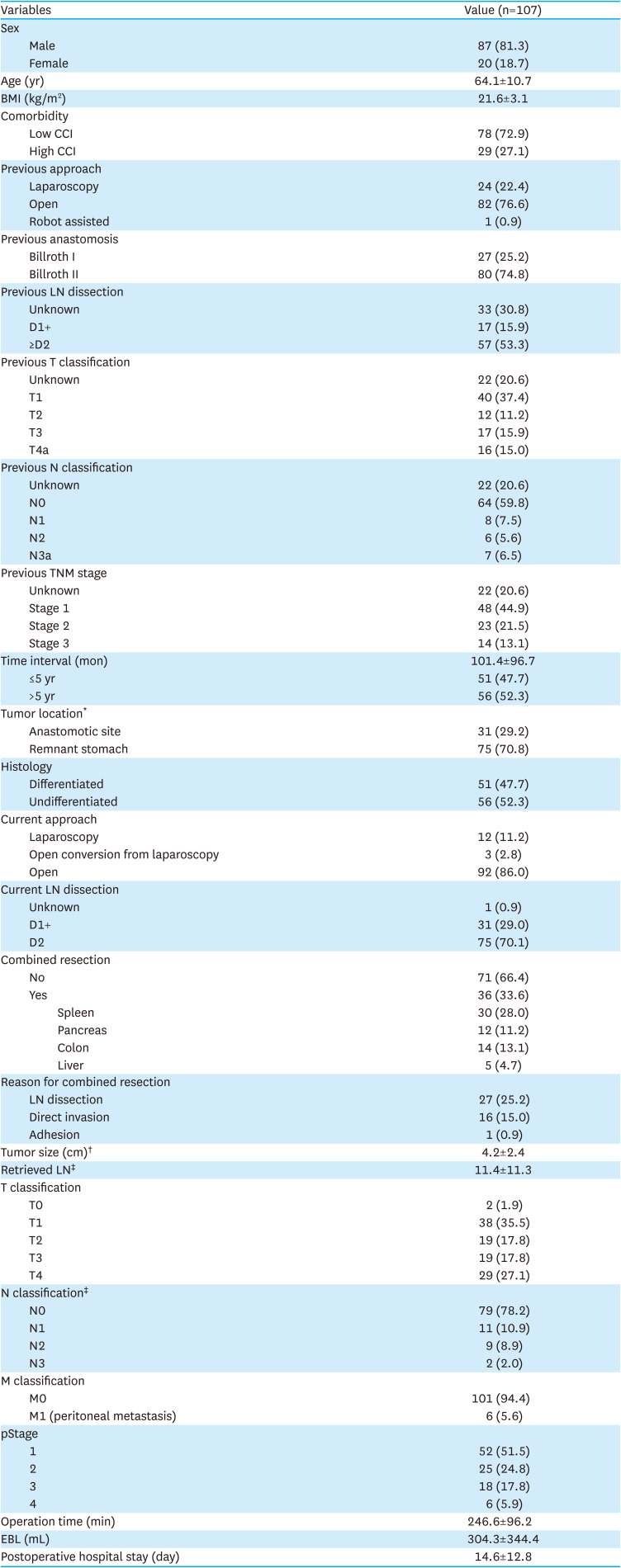
Materials and methods: We retrospectively reviewed the data of 107 patients who had previously undergone an initial gastric cancer surgery and subsequently underwent CTG for RGC between March 2002 and December 2020. The postoperative complications were graded using the Clavien-Dindo classification. Logistic regression analyses were used to determine the risk factors for complications.
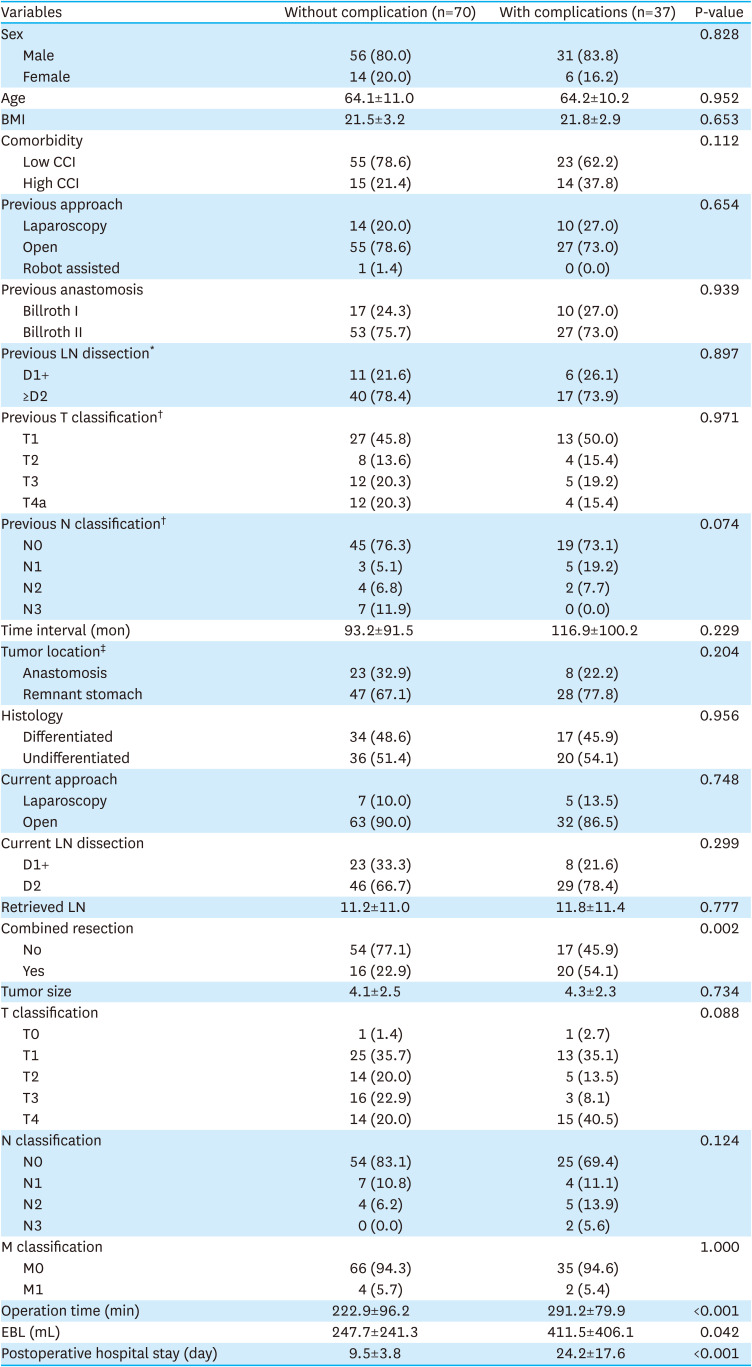
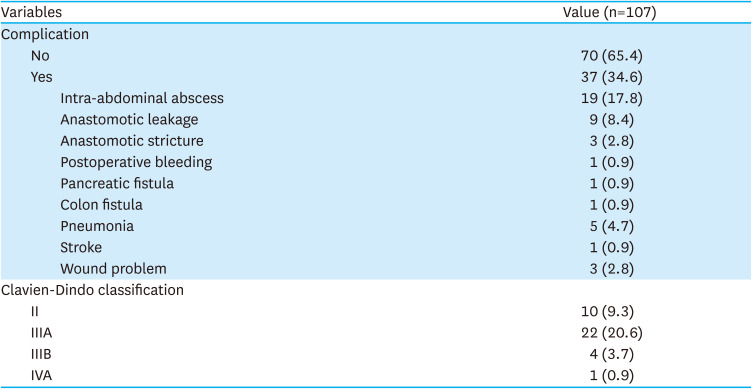
Results: Postoperative complications occurred in 34.6% (37/107) of the patients. Intra-abdominal abscess was the most common complication. The significant risk factors for overall complications were multi-visceral resections, longer operation time, and high estimated blood loss in the univariate analysis. The independent risk factors were multi-visceral resection (odds ratio [OR], 2.832; 95% confidence interval [CI], 1.094-7.333; P=0.032) and longer operation time (OR, 1.005; 95% CI, 1.001-1.011; P=0.036) in the multivariate analysis. Previous reconstruction type, minimally invasive approach, and current stage were not associated with the overall complications.
Conclusions: Multi-visceral resection and long operation time were significant risk factors for the occurrence of complications following CTG rather than the RGC stage or surgical approach. When multi-visceral resection is required, a more meticulous surgical procedure is warranted to improve the postoperative complications during CTG for RGC after an initial gastric cancer surgery.
期刊介绍:
The Journal of Gastric Cancer (J Gastric Cancer) is an international peer-reviewed journal. Each issue carries high quality clinical and translational researches on gastric neoplasms. Editorial Board of J Gastric Cancer publishes original articles on pathophysiology, molecular oncology, diagnosis, treatment, and prevention of gastric cancer as well as articles on dietary control and improving the quality of life for gastric cancer patients. J Gastric Cancer includes case reports, review articles, how I do it articles, editorials, and letters to the editor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


