Jill Carlton, Helen J Griffiths, Paolo Mazzone, Anna M Horwood, Frea Sloot
{"title":"A Comprehensive Overview of Vision Screening Programmes across 46 Countries.","authors":"Jill Carlton, Helen J Griffiths, Paolo Mazzone, Anna M Horwood, Frea Sloot","doi":"10.22599/bioj.260","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To describe and compare vision screening programmes and identify variance in number and type of tests used, timing of screening, personnel involved, monitoring and funding to be used as data for optimising, disinvesting or implementing future screening programmes.</p><p><strong>Methods: </strong>A questionnaire consisting of nine domains: demography & epidemiology, administration & general background, existing screening, coverage & attendance, tests, follow-up & diagnosis, treatment, cost & benefit and adverse effects was completed by Country Representatives (CRs) recruited from 47 countries.</p><p><strong>Results: </strong>The questionnaire was sufficiently completed for 46 Countries: 42 European countries, China, India, Malawi and Rwanda. Variation of provision was found in; age of screening (0-17 years), tests included (23), types of visual acuity (VA) test used (35 different optotypes), personnel (13), number of screens per child (median 5, range 1-32), and times VA tested (median 3, range 1-30). Infant screening is offered in all countries, whereas childhood vision screening is offered at least once in all countries, but not all regions of each country. All 46 countries provide vision screening between the ages of 3-7 years. Data on screening outcomes for quality assurance was not available from most countries; complete evaluation data was available in 2% of countries, partial data from 43%.</p><p><strong>Conclusion: </strong>Vision screening is highly variable. Some form of VA testing is being undertaken during childhood. Data collection and sharing should be improved to facilitate comparison and to be able to optimise vision screening programmes between regions and countries.</p>","PeriodicalId":36083,"journal":{"name":"British and Irish Orthoptic Journal","volume":" ","pages":"27-47"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9187246/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"British and Irish Orthoptic Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22599/bioj.260","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 3
Abstract
Purpose: To describe and compare vision screening programmes and identify variance in number and type of tests used, timing of screening, personnel involved, monitoring and funding to be used as data for optimising, disinvesting or implementing future screening programmes.
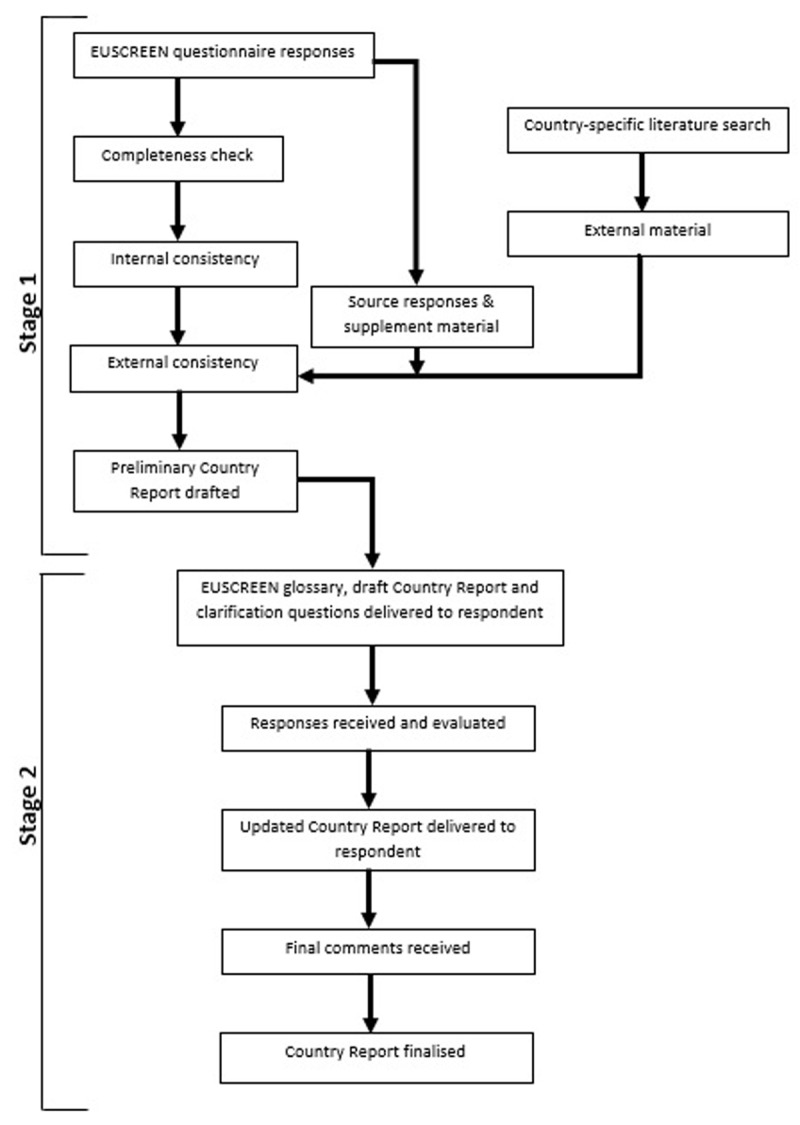
Methods: A questionnaire consisting of nine domains: demography & epidemiology, administration & general background, existing screening, coverage & attendance, tests, follow-up & diagnosis, treatment, cost & benefit and adverse effects was completed by Country Representatives (CRs) recruited from 47 countries.
Results: The questionnaire was sufficiently completed for 46 Countries: 42 European countries, China, India, Malawi and Rwanda. Variation of provision was found in; age of screening (0-17 years), tests included (23), types of visual acuity (VA) test used (35 different optotypes), personnel (13), number of screens per child (median 5, range 1-32), and times VA tested (median 3, range 1-30). Infant screening is offered in all countries, whereas childhood vision screening is offered at least once in all countries, but not all regions of each country. All 46 countries provide vision screening between the ages of 3-7 years. Data on screening outcomes for quality assurance was not available from most countries; complete evaluation data was available in 2% of countries, partial data from 43%.
Conclusion: Vision screening is highly variable. Some form of VA testing is being undertaken during childhood. Data collection and sharing should be improved to facilitate comparison and to be able to optimise vision screening programmes between regions and countries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


