Hu Li, Francis Mawanda, Lucy Mitchell, Xiang Zhang, Robert Goodloe, Maurice Vincent, Stephen Motsko
{"title":"Potential Channeling Bias in the Evaluation of Cardiovascular Risk: The Importance of Comparator Selection in Observational Research.","authors":"Hu Li, Francis Mawanda, Lucy Mitchell, Xiang Zhang, Robert Goodloe, Maurice Vincent, Stephen Motsko","doi":"10.1007/s40290-022-00433-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Comparator selection is an important consideration in the design of observational research studies that evaluate potential associations between drug therapies and adverse event risks. It can affect the validity of observational study results, and potentially impact data interpretation, regulatory decision making, and patient medication access.</p><p><strong>Objective: </strong>The aim of this study was to assess the impact of comparator selection bias using two real-world case studies evaluating an increased rate of acute myocardial infarction (AMI).</p><p><strong>Methods: </strong>Data from the Truven Health Analytics MarketScan<sup>®</sup> electronic medical claims database were used to conduct two retrospective observational cohort studies, utilizing a cohort new-user design, comparing AMI risk between testosterone replacement therapy (TRT) and phosphodiesterase-5 inhibitors (PDE5is) in men treated for hypogonadism, and triptans versus other prescribed acute treatments for migraine in adults. All patients were enrolled continuously in a health plan (no enrollment gap > 31 consecutive days) for ≥ 1 year before index. Baseline period was defined as 365 days prior to index. Exposure was defined by prescription and outcome of interest was defined as occurrence of AMI. Using Cox proportional hazard models, primary analysis for the TRT cohort compared AMI risk between propensity score (PS)-matched TRT-treated and untreated patients; secondary analysis evaluated risk between PS-matched TRT-treated and PDE5i-treated patients. For the triptan cohort, primary analysis compared AMI/ischemic stroke risk between PS-matched triptan-treated and opiate-treated patients; secondary analysis evaluated risk between PS-matched triptan-treated and nonsteroidal anti-inflammatory drug (NSAID)-treated patients and PS-matched non-prescription-treated migraine patients and general patients.</p><p><strong>Results: </strong>No significant association between TRT and AMI was observed among TRT-treated (N = 198,528, mean age 52.4 ± 11.4 years) versus PDE5i-treated men (N = 198,528, mean age 52.3 ± 11.5 years) overall (adjusted hazard ratio [aHR] 1.01; 95% CI 0.95-1.07; p = 0.80). Among patients with prior cardiovascular disease (CVD), risk of AMI was significantly increased for TRT-treated versus PDE5i-treated patients (aHR 1.13; 95% CI 1.03-1.25). The triptan study included three comparisons (triptans [N = 436,642] vs prescription NSAIDs [N = 334,152], opiates [N = 55,234], and untreated migraine [N = 1,168,212]), and a positive control (untreated vs general non-migraine patients [N = 11,735,009]). Analyses of MI risk in migraine patients prescribed triptans versus NSAIDs/opiates had mixed results: the point estimate ranged from 0.33 to 0.84 depending on chosen study window.</p><p><strong>Conclusions: </strong>Cardiovascular outcomes were not worse in hypogonadism patients with TRT versus PDE5i; however, a potential association with AMI was found in patients with prior CVD receiving TRT versus PDE5i. Findings pointed to a pseudo-protective effect of triptans versus untreated migraine patients or those potentially older and less healthy patients exposed to prescription NSAIDs or opiates. Triptan users should not be compared with those using other anti-migraine prescriptions when evaluating cardiovascular outcomes in migraine patients. Presence of high cardiovascular risks may contribute to channeling bias-healthier subjects being selected to receive treatment-highlighting the importance of choosing comparators wisely in observational studies.</p>","PeriodicalId":19778,"journal":{"name":"Pharmaceutical Medicine","volume":"36 4","pages":"247-259"},"PeriodicalIF":3.1000,"publicationDate":"2022-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6f/39/40290_2022_Article_433.PMC9334378.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmaceutical Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40290-022-00433-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/4 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Comparator selection is an important consideration in the design of observational research studies that evaluate potential associations between drug therapies and adverse event risks. It can affect the validity of observational study results, and potentially impact data interpretation, regulatory decision making, and patient medication access.
Objective: The aim of this study was to assess the impact of comparator selection bias using two real-world case studies evaluating an increased rate of acute myocardial infarction (AMI).
Methods: Data from the Truven Health Analytics MarketScan® electronic medical claims database were used to conduct two retrospective observational cohort studies, utilizing a cohort new-user design, comparing AMI risk between testosterone replacement therapy (TRT) and phosphodiesterase-5 inhibitors (PDE5is) in men treated for hypogonadism, and triptans versus other prescribed acute treatments for migraine in adults. All patients were enrolled continuously in a health plan (no enrollment gap > 31 consecutive days) for ≥ 1 year before index. Baseline period was defined as 365 days prior to index. Exposure was defined by prescription and outcome of interest was defined as occurrence of AMI. Using Cox proportional hazard models, primary analysis for the TRT cohort compared AMI risk between propensity score (PS)-matched TRT-treated and untreated patients; secondary analysis evaluated risk between PS-matched TRT-treated and PDE5i-treated patients. For the triptan cohort, primary analysis compared AMI/ischemic stroke risk between PS-matched triptan-treated and opiate-treated patients; secondary analysis evaluated risk between PS-matched triptan-treated and nonsteroidal anti-inflammatory drug (NSAID)-treated patients and PS-matched non-prescription-treated migraine patients and general patients.
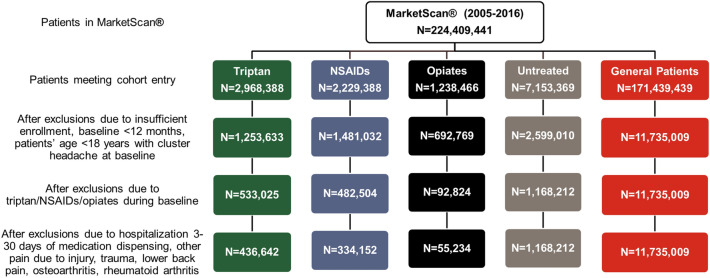
Results: No significant association between TRT and AMI was observed among TRT-treated (N = 198,528, mean age 52.4 ± 11.4 years) versus PDE5i-treated men (N = 198,528, mean age 52.3 ± 11.5 years) overall (adjusted hazard ratio [aHR] 1.01; 95% CI 0.95-1.07; p = 0.80). Among patients with prior cardiovascular disease (CVD), risk of AMI was significantly increased for TRT-treated versus PDE5i-treated patients (aHR 1.13; 95% CI 1.03-1.25). The triptan study included three comparisons (triptans [N = 436,642] vs prescription NSAIDs [N = 334,152], opiates [N = 55,234], and untreated migraine [N = 1,168,212]), and a positive control (untreated vs general non-migraine patients [N = 11,735,009]). Analyses of MI risk in migraine patients prescribed triptans versus NSAIDs/opiates had mixed results: the point estimate ranged from 0.33 to 0.84 depending on chosen study window.
Conclusions: Cardiovascular outcomes were not worse in hypogonadism patients with TRT versus PDE5i; however, a potential association with AMI was found in patients with prior CVD receiving TRT versus PDE5i. Findings pointed to a pseudo-protective effect of triptans versus untreated migraine patients or those potentially older and less healthy patients exposed to prescription NSAIDs or opiates. Triptan users should not be compared with those using other anti-migraine prescriptions when evaluating cardiovascular outcomes in migraine patients. Presence of high cardiovascular risks may contribute to channeling bias-healthier subjects being selected to receive treatment-highlighting the importance of choosing comparators wisely in observational studies.
期刊介绍:
Pharmaceutical Medicine is a specialist discipline concerned with medical aspects of the discovery, development, evaluation, registration, regulation, monitoring, marketing, distribution and pricing of medicines, drug-device and drug-diagnostic combinations. The Journal disseminates information to support the community of professionals working in these highly inter-related functions. Key areas include translational medicine, clinical trial design, pharmacovigilance, clinical toxicology, drug regulation, clinical pharmacology, biostatistics and pharmacoeconomics. The Journal includes:Overviews of contentious or emerging issues.Comprehensive narrative reviews that provide an authoritative source of information on topical issues.Systematic reviews that collate empirical evidence to answer a specific research question, using explicit, systematic methods as outlined by PRISMA statement.Original research articles reporting the results of well-designed studies with a strong link to wider areas of clinical research.Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in Pharmaceutical Medicine may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


