Kaipeng Duan, Dongbao Li, Dongtao Shi, Jie Pei, Jiayu Ren, Weikang Li, Anqi Dong, Tao Chen, Jin Zhou
{"title":"Risk Factors and Timing of Additional Surgery after Noncurative ESD for Early Gastric Cancer.","authors":"Kaipeng Duan, Dongbao Li, Dongtao Shi, Jie Pei, Jiayu Ren, Weikang Li, Anqi Dong, Tao Chen, Jin Zhou","doi":"10.1155/2022/3421078","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with early gastric cancer undergoing noncurative endoscopic submucosal dissection (ESD) have a risk of tumor recurrence and metastasis, and some patients need additional surgery. The purpose of this study was to explore the risk factors of cancer residue and lymph node (LN) metastasis after noncurative ESD for early gastric cancer and to compare the short outcome of early and delayed additional surgery.</p><p><strong>Methods: </strong>The clinicopathological characteristics of 30 early gastric cancer patients who received noncurative ESD and additional surgery were studied retrospectively. Multivariable regression was utilized to examine the independent risk factors for residual cancer and LN metastasis. Receiver operating characteristic curve was used to analyze the multivariable model's predictive performance. Furthermore, the perioperative safety and radical tumor performance of early surgery (≤30 days, <i>n</i> = 11), delayed surgery (>30 days, <i>n</i> = 11) after ESD, and upfront surgery (<i>n</i> = 59) were compared.</p><p><strong>Results: </strong>Multivariable regression showed that diffuse type of Lauren classification, submucosal invasion, and positive human epidermal growth factor receptor-2 (HER-2) were risk factors for residual cancer. Undifferentiated carcinoma, vascular invasion, and positive vertical margin were risk factors for LN metastasis. The area under the curve (AUC) of the multifactor model predicting cancer residue and LN metastasis was 0.761 and 0.792, respectively. The early surgery group experienced higher intraoperative blood loss and a longer operation time than the delayed surgery and upfront surgery groups. There was no significant difference in the number of LN dissections, LN metastasis rate, and postoperative complications among the three groups.</p><p><strong>Conclusion: </strong>Diffuse type of Lauren classification, submucosal invasion, and positive HER-2 are risk factors for residual cancer, while undifferentiated carcinoma, vascular invasion, and positive vertical margin are risk factors for LN metastasis. Delayed additional surgery after ESD (>30 days) has higher intraoperative safety, without affecting the radical resection in early gastric cancer patients.</p>","PeriodicalId":48755,"journal":{"name":"Canadian Journal of Gastroenterology and Hepatology","volume":" ","pages":"3421078"},"PeriodicalIF":2.7000,"publicationDate":"2022-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9239820/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Gastroenterology and Hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2022/3421078","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Patients with early gastric cancer undergoing noncurative endoscopic submucosal dissection (ESD) have a risk of tumor recurrence and metastasis, and some patients need additional surgery. The purpose of this study was to explore the risk factors of cancer residue and lymph node (LN) metastasis after noncurative ESD for early gastric cancer and to compare the short outcome of early and delayed additional surgery.
Methods: The clinicopathological characteristics of 30 early gastric cancer patients who received noncurative ESD and additional surgery were studied retrospectively. Multivariable regression was utilized to examine the independent risk factors for residual cancer and LN metastasis. Receiver operating characteristic curve was used to analyze the multivariable model's predictive performance. Furthermore, the perioperative safety and radical tumor performance of early surgery (≤30 days, n = 11), delayed surgery (>30 days, n = 11) after ESD, and upfront surgery (n = 59) were compared.
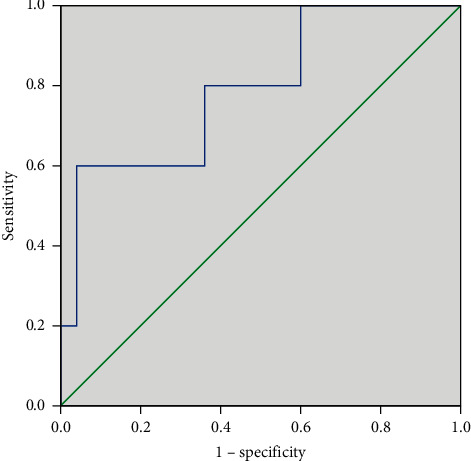
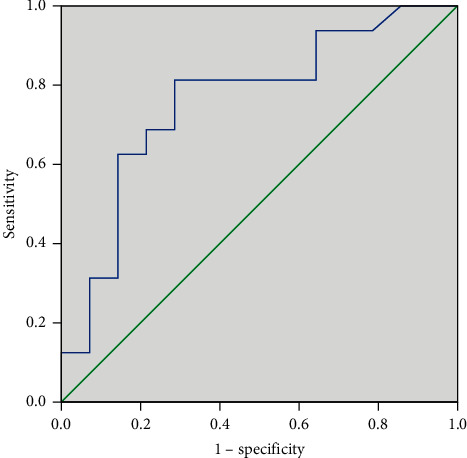
Results: Multivariable regression showed that diffuse type of Lauren classification, submucosal invasion, and positive human epidermal growth factor receptor-2 (HER-2) were risk factors for residual cancer. Undifferentiated carcinoma, vascular invasion, and positive vertical margin were risk factors for LN metastasis. The area under the curve (AUC) of the multifactor model predicting cancer residue and LN metastasis was 0.761 and 0.792, respectively. The early surgery group experienced higher intraoperative blood loss and a longer operation time than the delayed surgery and upfront surgery groups. There was no significant difference in the number of LN dissections, LN metastasis rate, and postoperative complications among the three groups.
Conclusion: Diffuse type of Lauren classification, submucosal invasion, and positive HER-2 are risk factors for residual cancer, while undifferentiated carcinoma, vascular invasion, and positive vertical margin are risk factors for LN metastasis. Delayed additional surgery after ESD (>30 days) has higher intraoperative safety, without affecting the radical resection in early gastric cancer patients.
期刊介绍:
Canadian Journal of Gastroenterology and Hepatology is a peer-reviewed, open access journal that publishes original research articles, review articles, and clinical studies in all areas of gastroenterology and liver disease - medicine and surgery.
The Canadian Journal of Gastroenterology and Hepatology is sponsored by the Canadian Association of Gastroenterology and the Canadian Association for the Study of the Liver.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


