Francesco Lorusso, Francesco Dispenza, Federico Sireci, Angelo Immordino, Palmira Immordino, Salvatore Gallina
{"title":"Management of pharyngeal collapse in patients affected by moderate obstructive sleep apnoea syndrome.","authors":"Francesco Lorusso, Francesco Dispenza, Federico Sireci, Angelo Immordino, Palmira Immordino, Salvatore Gallina","doi":"10.14639/0392-100X-N1871","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study reports our experience in a selected cohort of patients affected by mild-moderate OSAS, without tonsillar obstruction, and treated with pharyngoplasty.</p><p><strong>Methods: </strong>In a case-control retrospective study, we compared modified expansion sphincter pharyngoplasty (MESP) to modified barbed reposition pharyngoplasty (MBRP) in adult patients with oropharyngeal transversal collapse with a BMI ≤ 30 kg/m<sup>2</sup>, and mild-moderate obstructive sleep apnoea syndrome (OSAS). A clinical evaluation, including collection of anthropometric data and sleep endoscopy, was performed. Six months after surgery, symptoms recording, clinical evaluation and polysomnography (PSG) were repeated.</p><p><strong>Results: </strong>We enrolled 20 patients: 10 treated with MESP and 10 treated with MBRP. Mean apnoea-hypoapnoea index (AHI) was 22.8 (± 5.63). We observed in both groups a significant reduction of AHI and oropharyngeal obstruction (p = 0.01), with a success rate, according with Sher's criteria, of 90% for MESP and 80% for MBRP, respectively. Post-surgical pain and snoring reduction were significantly lower with MBRP.</p><p><strong>Conclusions: </strong>We recorded similar success rates for both techniques. MBRP may be considered better than MESP due to less surgical time, no potential mucosal damage, absence of knots, and faster recovery with less pain.</p>","PeriodicalId":520544,"journal":{"name":"Acta otorhinolaryngologica Italica : organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale","volume":" ","pages":"273-280"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/68/17/aoi-2022-03-273.PMC9330758.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta otorhinolaryngologica Italica : organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14639/0392-100X-N1871","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Objective: This study reports our experience in a selected cohort of patients affected by mild-moderate OSAS, without tonsillar obstruction, and treated with pharyngoplasty.
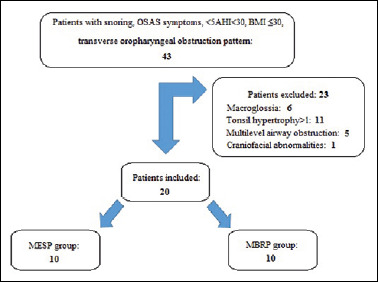
Methods: In a case-control retrospective study, we compared modified expansion sphincter pharyngoplasty (MESP) to modified barbed reposition pharyngoplasty (MBRP) in adult patients with oropharyngeal transversal collapse with a BMI ≤ 30 kg/m2, and mild-moderate obstructive sleep apnoea syndrome (OSAS). A clinical evaluation, including collection of anthropometric data and sleep endoscopy, was performed. Six months after surgery, symptoms recording, clinical evaluation and polysomnography (PSG) were repeated.
Results: We enrolled 20 patients: 10 treated with MESP and 10 treated with MBRP. Mean apnoea-hypoapnoea index (AHI) was 22.8 (± 5.63). We observed in both groups a significant reduction of AHI and oropharyngeal obstruction (p = 0.01), with a success rate, according with Sher's criteria, of 90% for MESP and 80% for MBRP, respectively. Post-surgical pain and snoring reduction were significantly lower with MBRP.
Conclusions: We recorded similar success rates for both techniques. MBRP may be considered better than MESP due to less surgical time, no potential mucosal damage, absence of knots, and faster recovery with less pain.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


