Cameron Dockerill, Harminder Gill, Joao Filipe Fernandes, Amanda Q X Nio, Ronak Rajani, Pablo Lamata
{"title":"Blood speckle imaging compared with conventional Doppler ultrasound for transvalvular pressure drop estimation in an aortic flow phantom.","authors":"Cameron Dockerill, Harminder Gill, Joao Filipe Fernandes, Amanda Q X Nio, Ronak Rajani, Pablo Lamata","doi":"10.1186/s12947-022-00286-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transvalvular pressure drops are assessed using Doppler echocardiography for the diagnosis of heart valve disease. However, this method is highly user-dependent and may overestimate transvalvular pressure drops by up to 54%. This work aimed to assess transvalvular pressure drops using velocity fields derived from blood speckle imaging (BSI), as a potential alternative to Doppler. METHODS: A silicone 3D-printed aortic valve model, segmented from a healthy CT scan, was placed within a silicone tube. A CardioFlow 5000MR flow pump was used to circulate blood mimicking fluid to create eight different stenotic conditions. Eight PendoTech pressure sensors were embedded along the tube wall to record ground-truth pressures (10 kHz). The simplified Bernoulli equation with measured probe angle correction was used to estimate pressure drop from maximum velocity values acquired across the valve using Doppler and BSI with a GE Vivid E95 ultrasound machine and 6S-D cardiac phased array transducer.</p><p><strong>Results: </strong>There were no significant differences between pressure drops estimated by Doppler, BSI and ground-truth at the lowest stenotic condition (10.4 ± 1.76, 10.3 ± 1.63 vs. 10.5 ± 1.00 mmHg, respectively; p > 0.05). Significant differences were observed between the pressure drops estimated by the three methods at the greatest stenotic condition (26.4 ± 1.52, 14.5 ± 2.14 vs. 20.9 ± 1.92 mmHg for Doppler, BSI and ground-truth, respectively; p < 0.05). Across all conditions, Doppler overestimated pressure drop (Bias = 3.92 mmHg), while BSI underestimated pressure drop (Bias = -3.31 mmHg).</p><p><strong>Conclusions: </strong>BSI accurately estimated pressure drops only up to 10.5 mmHg in controlled phantom conditions of low stenotic burden. Doppler overestimated pressure drops of 20.9 mmHg. Although BSI offers a number of theoretical advantages to conventional Doppler echocardiography, further refinements and clinical studies are required with BSI before it can be used to improve transvalvular pressure drop estimation in the clinical evaluation of aortic stenosis.</p>","PeriodicalId":9613,"journal":{"name":"Cardiovascular Ultrasound","volume":" ","pages":"18"},"PeriodicalIF":1.6000,"publicationDate":"2022-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9287947/pdf/","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Ultrasound","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12947-022-00286-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 4
Abstract
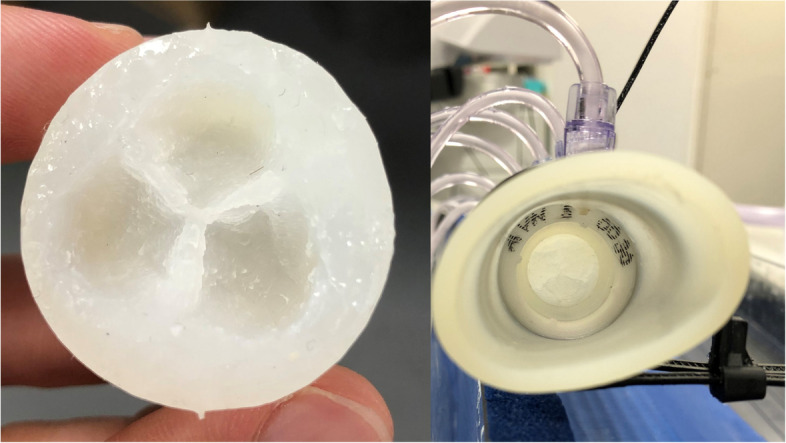
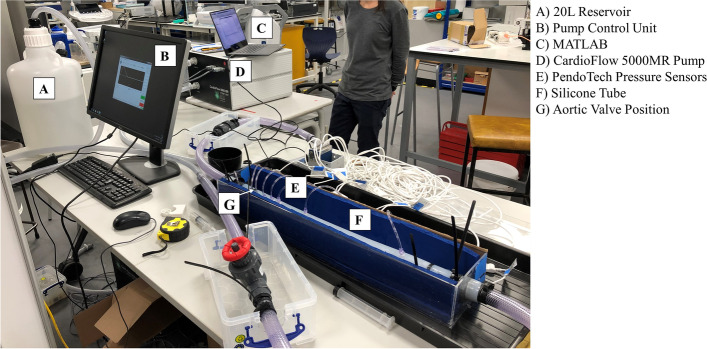
Background: Transvalvular pressure drops are assessed using Doppler echocardiography for the diagnosis of heart valve disease. However, this method is highly user-dependent and may overestimate transvalvular pressure drops by up to 54%. This work aimed to assess transvalvular pressure drops using velocity fields derived from blood speckle imaging (BSI), as a potential alternative to Doppler. METHODS: A silicone 3D-printed aortic valve model, segmented from a healthy CT scan, was placed within a silicone tube. A CardioFlow 5000MR flow pump was used to circulate blood mimicking fluid to create eight different stenotic conditions. Eight PendoTech pressure sensors were embedded along the tube wall to record ground-truth pressures (10 kHz). The simplified Bernoulli equation with measured probe angle correction was used to estimate pressure drop from maximum velocity values acquired across the valve using Doppler and BSI with a GE Vivid E95 ultrasound machine and 6S-D cardiac phased array transducer.
Results: There were no significant differences between pressure drops estimated by Doppler, BSI and ground-truth at the lowest stenotic condition (10.4 ± 1.76, 10.3 ± 1.63 vs. 10.5 ± 1.00 mmHg, respectively; p > 0.05). Significant differences were observed between the pressure drops estimated by the three methods at the greatest stenotic condition (26.4 ± 1.52, 14.5 ± 2.14 vs. 20.9 ± 1.92 mmHg for Doppler, BSI and ground-truth, respectively; p < 0.05). Across all conditions, Doppler overestimated pressure drop (Bias = 3.92 mmHg), while BSI underestimated pressure drop (Bias = -3.31 mmHg).
Conclusions: BSI accurately estimated pressure drops only up to 10.5 mmHg in controlled phantom conditions of low stenotic burden. Doppler overestimated pressure drops of 20.9 mmHg. Although BSI offers a number of theoretical advantages to conventional Doppler echocardiography, further refinements and clinical studies are required with BSI before it can be used to improve transvalvular pressure drop estimation in the clinical evaluation of aortic stenosis.
期刊介绍:
Cardiovascular Ultrasound is an online journal, publishing peer-reviewed: original research; authoritative reviews; case reports on challenging and/or unusual diagnostic aspects; and expert opinions on new techniques and technologies. We are particularly interested in articles that include relevant images or video files, which provide an additional dimension to published articles and enhance understanding.
As an open access journal, Cardiovascular Ultrasound ensures high visibility for authors in addition to providing an up-to-date and freely available resource for the community. The journal welcomes discussion, and provides a forum for publishing opinion and debate ranging from biology to engineering to clinical echocardiography, with both speed and versatility.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


