Joao Leote, Tiago Judas, Ana Luísa Broa, Miguel Lopes, Francisca Abecasis, Inês Pintassilgo, Afonso Gonçalves, Filipe Gonzalez
{"title":"Time course of lung ultrasound findings in patients with COVID-19 pneumonia and cardiac dysfunction.","authors":"Joao Leote, Tiago Judas, Ana Luísa Broa, Miguel Lopes, Francisca Abecasis, Inês Pintassilgo, Afonso Gonçalves, Filipe Gonzalez","doi":"10.1186/s13089-022-00278-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lung ultrasound (LUS) is a valuable tool to predict and monitor the COVID-19 pneumonia course. However, the influence of cardiac dysfunction (CD) on LUS findings remains to be studied. Our objective was to determine the effect of CD on LUS in hospitalized patients with COVID-19 pneumonia.</p><p><strong>Material and methods: </strong>Fifty-one patients with COVID-19 pneumonia participated in the study. Focused echocardiography (FoCUS) was carried out on day 1 to separate patients into two groups depending on whether they had FoCUS signs of CD (CD+ vs CD-). LUS scores, based on the thickness of the pleural line, the B-line characteristics, and the presence or not of consolidations, were obtained three times along the patient's admission (D1, D5, D10) and compared between CD+ and CD- patients. A correlation analysis was carried out between LUS scores and the ratio of the arterial partial pressure of oxygen to the fraction of the inspired oxygen (P/F ratio).</p><p><strong>Results: </strong>Twenty-two patients were CD+ and 29 patients were CD-. Among the CD+ patients, 19 were admitted to the intensive care unit (ICU), seven received invasive mechanical ventilation (IMV), and one did not survive. Among the CD- patients, 11 were admitted to the ICU, one received IMV and seven did not survive. CD+ patients showed a significantly lower P/F ratio than CD- patients. However, LUS scores showed no between-group differences, except for fewer subpleural consolidations in the upper quadrants of CD+ than on CD- patients.</p><p><strong>Conclusion: </strong>In patients with COVID-19, CD contributed to a worse clinical course, but it did not induce significant changes in LUS. Our findings suggest that pathophysiological factors other than those reflected by LUS may be responsible for the differences in clinical condition between CD+ and CD- patients.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":" ","pages":"28"},"PeriodicalIF":3.4000,"publicationDate":"2022-07-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9261145/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-022-00278-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Lung ultrasound (LUS) is a valuable tool to predict and monitor the COVID-19 pneumonia course. However, the influence of cardiac dysfunction (CD) on LUS findings remains to be studied. Our objective was to determine the effect of CD on LUS in hospitalized patients with COVID-19 pneumonia.
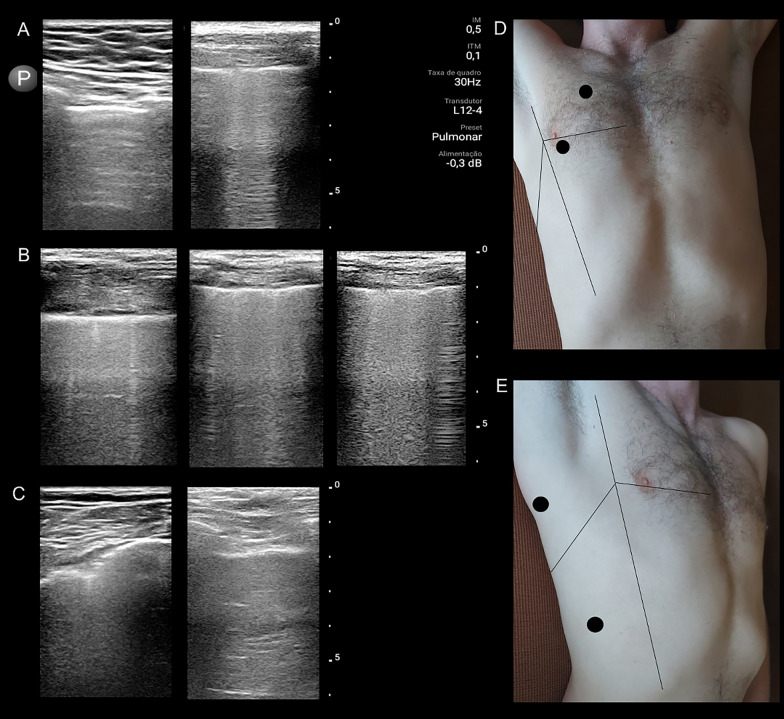
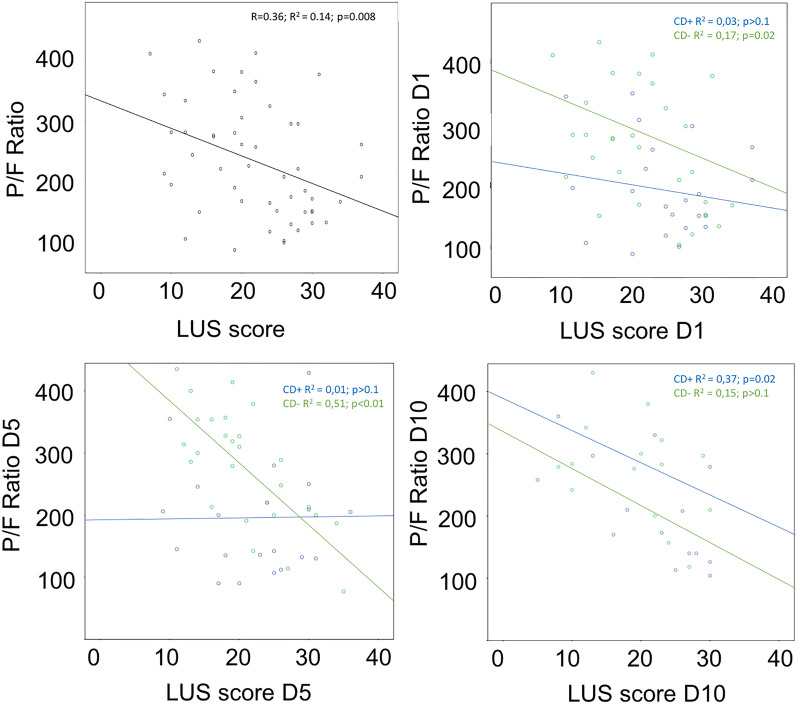
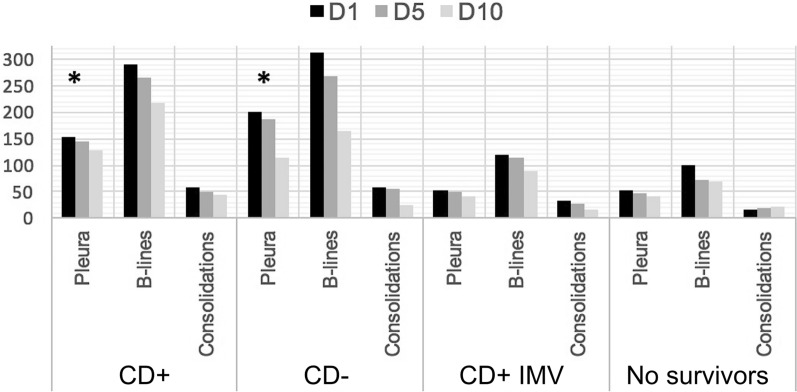
Material and methods: Fifty-one patients with COVID-19 pneumonia participated in the study. Focused echocardiography (FoCUS) was carried out on day 1 to separate patients into two groups depending on whether they had FoCUS signs of CD (CD+ vs CD-). LUS scores, based on the thickness of the pleural line, the B-line characteristics, and the presence or not of consolidations, were obtained three times along the patient's admission (D1, D5, D10) and compared between CD+ and CD- patients. A correlation analysis was carried out between LUS scores and the ratio of the arterial partial pressure of oxygen to the fraction of the inspired oxygen (P/F ratio).
Results: Twenty-two patients were CD+ and 29 patients were CD-. Among the CD+ patients, 19 were admitted to the intensive care unit (ICU), seven received invasive mechanical ventilation (IMV), and one did not survive. Among the CD- patients, 11 were admitted to the ICU, one received IMV and seven did not survive. CD+ patients showed a significantly lower P/F ratio than CD- patients. However, LUS scores showed no between-group differences, except for fewer subpleural consolidations in the upper quadrants of CD+ than on CD- patients.
Conclusion: In patients with COVID-19, CD contributed to a worse clinical course, but it did not induce significant changes in LUS. Our findings suggest that pathophysiological factors other than those reflected by LUS may be responsible for the differences in clinical condition between CD+ and CD- patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


