Gabriel Martins Nogueira, Noel Lucas Oliveira Rodrigues Silva, Ana Flávia Moura, Marcelo Augusto Duarte Silveira, José A Moura-Neto
{"title":"Acute kidney injury and electrolyte disorders in COVID-19.","authors":"Gabriel Martins Nogueira, Noel Lucas Oliveira Rodrigues Silva, Ana Flávia Moura, Marcelo Augusto Duarte Silveira, José A Moura-Neto","doi":"10.5501/wjv.v11.i5.283","DOIUrl":null,"url":null,"abstract":"<p><p>Acute kidney injury (AKI) and electrolyte disorders are important complications of hospitalized coronavirus disease 2019 (COVID-19) patients. AKI is thought to occur due to multiple pathophysiological mechanisms, such as multiple organ dysfunction (mainly cardiac and respiratory), direct viral entry in the renal tubules, and cytokine release syndrome. AKI is present in approximately one in every ten hospitalized COVID-19 patients. The incidence rates of AKI increase in patients who are admitted to the intensive care unit (ICU), with levels higher than 50%. Additionally, renal replacement therapy (RRT) is used in 7% of all AKI cases, but in nearly 20% of patients admitted to an ICU. COVID-19 patients with AKI are considered moderate-to-severe cases and are managed with multiple interdisciplinary conducts. AKI acts as a risk factor for mortality in severe acute respiratory syndrome coronavirus 2 infection, especially when RRT is needed. Electrolyte disorders are also common manifestations in hospitalized COVID-19 patients, mainly hyponatremia, hypokalemia, and hypocalcemia. Hyponatremia occurs due to a combination of syndrome of inappropriate secretion of antidiuretic hormone and gastrointestinal fluid loss from vomiting and diarrhea. When it comes to hypokalemia, its mechanism is not fully understood but may derive from hyperaldosteronism due to renin angiotensin aldosterone system overstimulation and gastrointestinal fluid loss as well. The clinical features of hypokalemia in COVID-19 are similar to those in other conditions. Hypocalcemia is the most common electrolyte disorder in COVID-19 and seems to occur because of vitamin D deficiency and parathyroid imbalance. It is also highly associated with longer hospital and ICU stay.</p>","PeriodicalId":61903,"journal":{"name":"世界病毒学杂志(英文版)","volume":"11 5","pages":"283-292"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8d/1e/WJV-11-283.PMC9523327.pdf","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界病毒学杂志(英文版)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5501/wjv.v11.i5.283","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
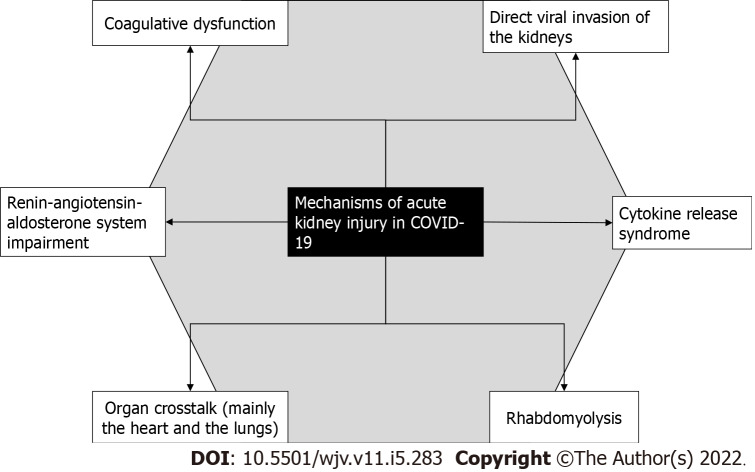
Acute kidney injury (AKI) and electrolyte disorders are important complications of hospitalized coronavirus disease 2019 (COVID-19) patients. AKI is thought to occur due to multiple pathophysiological mechanisms, such as multiple organ dysfunction (mainly cardiac and respiratory), direct viral entry in the renal tubules, and cytokine release syndrome. AKI is present in approximately one in every ten hospitalized COVID-19 patients. The incidence rates of AKI increase in patients who are admitted to the intensive care unit (ICU), with levels higher than 50%. Additionally, renal replacement therapy (RRT) is used in 7% of all AKI cases, but in nearly 20% of patients admitted to an ICU. COVID-19 patients with AKI are considered moderate-to-severe cases and are managed with multiple interdisciplinary conducts. AKI acts as a risk factor for mortality in severe acute respiratory syndrome coronavirus 2 infection, especially when RRT is needed. Electrolyte disorders are also common manifestations in hospitalized COVID-19 patients, mainly hyponatremia, hypokalemia, and hypocalcemia. Hyponatremia occurs due to a combination of syndrome of inappropriate secretion of antidiuretic hormone and gastrointestinal fluid loss from vomiting and diarrhea. When it comes to hypokalemia, its mechanism is not fully understood but may derive from hyperaldosteronism due to renin angiotensin aldosterone system overstimulation and gastrointestinal fluid loss as well. The clinical features of hypokalemia in COVID-19 are similar to those in other conditions. Hypocalcemia is the most common electrolyte disorder in COVID-19 and seems to occur because of vitamin D deficiency and parathyroid imbalance. It is also highly associated with longer hospital and ICU stay.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


