Vipul D Yagnik, Baljit Kaur, Sushil Dawka, Aalam Sohal, Geetha R Menon, Pankaj Garg
{"title":"Non-Locatable Internal Opening in Anal Fistula Associated with Acute Abscess and Its Definitive Management by Garg Protocol.","authors":"Vipul D Yagnik, Baljit Kaur, Sushil Dawka, Aalam Sohal, Geetha R Menon, Pankaj Garg","doi":"10.2147/CEG.S374848","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Definitive management of acute fistula-abscess (anal fistulas associated with acute abscess) is gaining popularity against the two-staged approach (early abscess drainage with deferred fistula management). However, locating an internal opening (IO) in acute fistula-abscess can be difficult. A recent protocol (Garg protocol) has been shown to be effective in managing anal fistulas with non-locatable IO.</p><p><strong>Purpose: </strong>To test the efficacy of the Garg protocol in managing acute fistula-abscess with non-locatable IO.</p><p><strong>Methods: </strong>Patients with acute fistula-abscess operated by a definitive procedure were included. A preoperative MRI was done in all patients. Patients in whom the IO was non-locatable after clinical, MRI, and intraoperative examination were managed by the three-step Garg protocol. Garg protocol: 1) Reassessment of MRI; 2) In non-horseshoe fistulas, the IO was assumed to be at the point where the fistula tract reached closest to the sphincter-complex; 3) In horseshoe fistulas, the IO was assumed to be located in the midline (anterior or posterior as per the horseshoe location). Low fistulas were treated by fistulotomy and high fistulas by a sphincter-sparing procedure. The long-term healing rate and change in continence (Vaizey scores) were evaluated.</p><p><strong>Results: </strong>A total of 201 patients with acute fistula-abscess were operated over six years, and 19 were lost to follow-up. A total of 182 patients (154-males) were followed up (median-37 months). The IO was locatable in 133/182 (73.1%) (control group) and was non-locatable in 49/182 (26.9%) (study group). The study group was managed as per the Garg protocol. The age, sex-ratio, and fistula parameters were comparable in both groups. The long-term healing rate was 112/133(84.2%) in the IO-locatable group and 43/49 (87.8%) in the IO-non-locatable group (p=0.64, not-significant). The objective continence scores did not change significantly after surgery in both groups.</p><p><strong>Conclusion: </strong>Acute fistula-abscess with non-locatable IO can be managed successfully by the Garg protocol without any risk of incontinence.</p>","PeriodicalId":10208,"journal":{"name":"Clinical and Experimental Gastroenterology","volume":" ","pages":"189-198"},"PeriodicalIF":2.5000,"publicationDate":"2022-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/00/41/ceg-15-189.PMC9525211.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Experimental Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEG.S374848","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Definitive management of acute fistula-abscess (anal fistulas associated with acute abscess) is gaining popularity against the two-staged approach (early abscess drainage with deferred fistula management). However, locating an internal opening (IO) in acute fistula-abscess can be difficult. A recent protocol (Garg protocol) has been shown to be effective in managing anal fistulas with non-locatable IO.
Purpose: To test the efficacy of the Garg protocol in managing acute fistula-abscess with non-locatable IO.
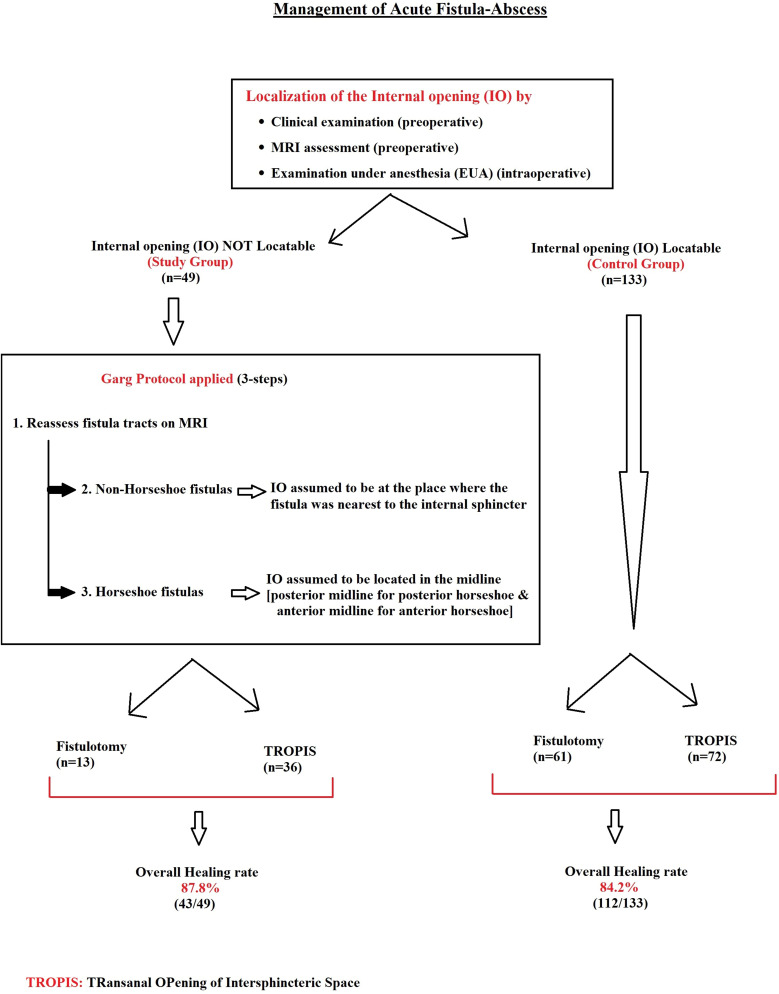
Methods: Patients with acute fistula-abscess operated by a definitive procedure were included. A preoperative MRI was done in all patients. Patients in whom the IO was non-locatable after clinical, MRI, and intraoperative examination were managed by the three-step Garg protocol. Garg protocol: 1) Reassessment of MRI; 2) In non-horseshoe fistulas, the IO was assumed to be at the point where the fistula tract reached closest to the sphincter-complex; 3) In horseshoe fistulas, the IO was assumed to be located in the midline (anterior or posterior as per the horseshoe location). Low fistulas were treated by fistulotomy and high fistulas by a sphincter-sparing procedure. The long-term healing rate and change in continence (Vaizey scores) were evaluated.
Results: A total of 201 patients with acute fistula-abscess were operated over six years, and 19 were lost to follow-up. A total of 182 patients (154-males) were followed up (median-37 months). The IO was locatable in 133/182 (73.1%) (control group) and was non-locatable in 49/182 (26.9%) (study group). The study group was managed as per the Garg protocol. The age, sex-ratio, and fistula parameters were comparable in both groups. The long-term healing rate was 112/133(84.2%) in the IO-locatable group and 43/49 (87.8%) in the IO-non-locatable group (p=0.64, not-significant). The objective continence scores did not change significantly after surgery in both groups.
Conclusion: Acute fistula-abscess with non-locatable IO can be managed successfully by the Garg protocol without any risk of incontinence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


