Long Wang, Xuegang Li, Tunan Chen, Chao Zhang, Jiantao Shi, Hua Feng, Fei Li
{"title":"Risk factors for early progression of diffuse low-grade glioma in adults.","authors":"Long Wang, Xuegang Li, Tunan Chen, Chao Zhang, Jiantao Shi, Hua Feng, Fei Li","doi":"10.1186/s41016-022-00295-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To explore the risk factors for early progression of diffuse low-grade glioma in adults.</p><p><strong>Methods: </strong>A retrospective analysis of pathologic and clinical data of patients diagnosed with diffuse low-grade gliomas at Southwest Hospital between January 2010 and December 2014. The progression-free survival (PFS) less than 60 months was classified as the early progress group, and the PFS greater than 60 months was the control group for comparative analysis.</p><p><strong>Results: </strong>A total of 138 patients were included in this study, including 94 cases of astrocytoma and 44 cases of oligodendroglioma. There were 63 cases with 100% resection, 56 cases with 90-100% resection degree, and 19 cases with resection degree < 90%. The average follow-up time was 60 months, of which 80 patients progressed and 58 patients did not progress. The average progression-free survival was 61 months. The median progression-free survival was 60 months. There were 68 patients with PFS ≤ 60 months and 70 patients with PFS > 60 months. The two groups were compared for statistical analysis. In univariate analysis, there were significant differences in tumor subtype (p = 0.005), range (p = 0.011), volume (p = 0.005), location (p = 0.000), and extent of resection (p = 0.000). Multifactor analysis shows tumor location (HR = 4.549, 95% CI: 1.324-15.634, p = 0.016) and tumor subtype (HR = 3.347, 95% CI = 1.373-8.157, p = 0.008), and imcomplete resection is factors influencing early progression of low-grade glioma.</p><p><strong>Conclusions: </strong>Low-grade gliomas involving deep location such as basal ganglia, inner capsule, and corpus callosum are more likely to progress early, while incomplete resection is a risk factor in early progression of astrocytoma.</p>","PeriodicalId":36700,"journal":{"name":"Chinese Neurosurgical Journal","volume":" ","pages":"25"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9526265/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chinese Neurosurgical Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s41016-022-00295-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: To explore the risk factors for early progression of diffuse low-grade glioma in adults.
Methods: A retrospective analysis of pathologic and clinical data of patients diagnosed with diffuse low-grade gliomas at Southwest Hospital between January 2010 and December 2014. The progression-free survival (PFS) less than 60 months was classified as the early progress group, and the PFS greater than 60 months was the control group for comparative analysis.
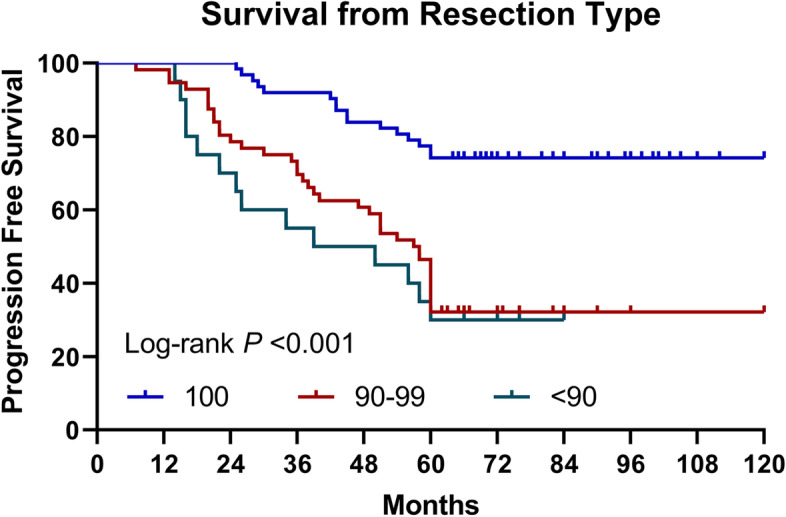
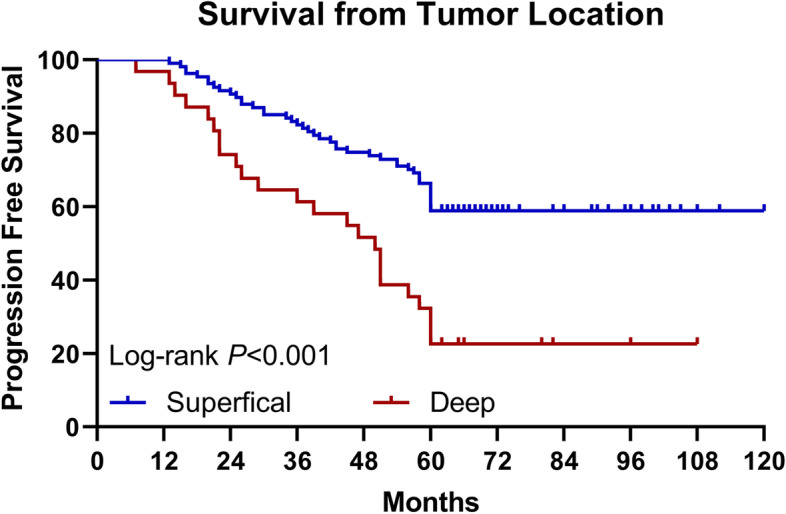
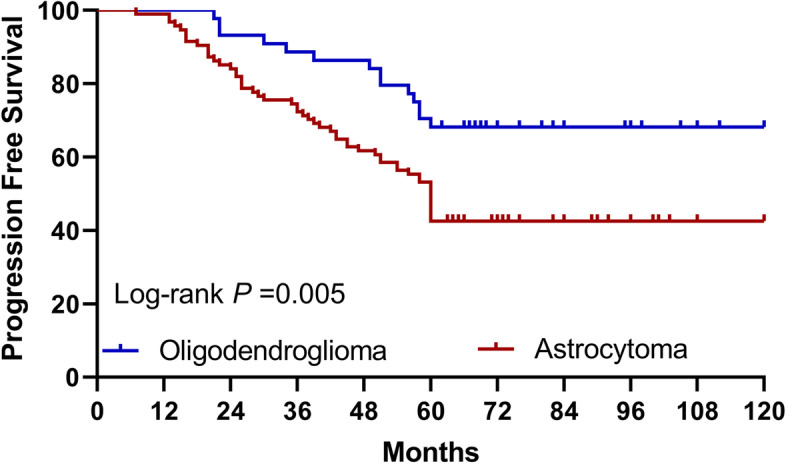
Results: A total of 138 patients were included in this study, including 94 cases of astrocytoma and 44 cases of oligodendroglioma. There were 63 cases with 100% resection, 56 cases with 90-100% resection degree, and 19 cases with resection degree < 90%. The average follow-up time was 60 months, of which 80 patients progressed and 58 patients did not progress. The average progression-free survival was 61 months. The median progression-free survival was 60 months. There were 68 patients with PFS ≤ 60 months and 70 patients with PFS > 60 months. The two groups were compared for statistical analysis. In univariate analysis, there were significant differences in tumor subtype (p = 0.005), range (p = 0.011), volume (p = 0.005), location (p = 0.000), and extent of resection (p = 0.000). Multifactor analysis shows tumor location (HR = 4.549, 95% CI: 1.324-15.634, p = 0.016) and tumor subtype (HR = 3.347, 95% CI = 1.373-8.157, p = 0.008), and imcomplete resection is factors influencing early progression of low-grade glioma.
Conclusions: Low-grade gliomas involving deep location such as basal ganglia, inner capsule, and corpus callosum are more likely to progress early, while incomplete resection is a risk factor in early progression of astrocytoma.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


