David Dreizin, Theresa Yu, Kaitlynn Motley, Guang Li, Jonathan J Morrison, Yuanyuan Liang
{"title":"Blunt splenic injury: Assessment of follow-up CT utility using quantitative volumetry.","authors":"David Dreizin, Theresa Yu, Kaitlynn Motley, Guang Li, Jonathan J Morrison, Yuanyuan Liang","doi":"10.3389/fradi.2022.941863","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Trials of non-operative management (NOM) have become the standard of care for blunt splenic injury (BSI) in hemodynamically stable patients. However, there is a lack of consensus regarding the utility of follow-up CT exams and relevant CT features. The purpose of this study is to determine imaging predictors of splenectomy on follow-up CT using quantitative volumetric measurements.</p><p><strong>Methods: </strong>Adult patients who underwent a trial of non-operative management (NOM) with follow-up CT performed for BSI between 2017 and 2019 were included (<i>n</i> = 51). Six patients (12% of cohort) underwent splenectomy; 45 underwent successful splenic salvage. Voxelwise measurements of splenic laceration, hemoperitoneum, and subcapsular hematoma were derived from portal venous phase images of admission and follow-up scans using 3D slicer. Presence/absence of pseudoaneurysm on admission and follow-up CT was assessed using arterial phase images. Multivariable logistic regression was used to determine independent predictors of decision to perform splenectomy.</p><p><strong>Results: </strong>Factors significantly associated with splenectomy in bivariate analysis incorporated in multivariate logistic regression included final hemoperitoneum volume (<i>p</i> = 0.003), final subcapsular hematoma volume (<i>p</i> = 0.001), change in subcapsular hematoma volume between scans (<i>p</i> = 0.09) and new/persistent pseudoaneurysm (<i>p</i> = 0.003). Independent predictors of splenectomy in the logistic regression were final hemoperitoneum volume (unit OR = 1.43 for each 100 mL change; 95% CI: 0.99-2.06) and new/persistent pseudoaneurysm (OR = 160.3; 95% CI: 0.91-28315.3). The AUC of the model incorporating both variables was significantly higher than AAST grading (0.91 vs. 0.59, <i>p</i> = 0.025). Mean combined effective dose for admission and follow up CT scans was 37.4 mSv.</p><p><strong>Conclusion: </strong>Follow-up CT provides clinically valuable information regarding the decision to perform splenectomy in BSI patients managed non-operatively. Hemoperitoneum volume and new or persistent pseudoaneurysm at follow-up are independent predictors of splenectomy.</p>","PeriodicalId":73101,"journal":{"name":"Frontiers in radiology","volume":" ","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9479763/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fradi.2022.941863","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Purpose: Trials of non-operative management (NOM) have become the standard of care for blunt splenic injury (BSI) in hemodynamically stable patients. However, there is a lack of consensus regarding the utility of follow-up CT exams and relevant CT features. The purpose of this study is to determine imaging predictors of splenectomy on follow-up CT using quantitative volumetric measurements.
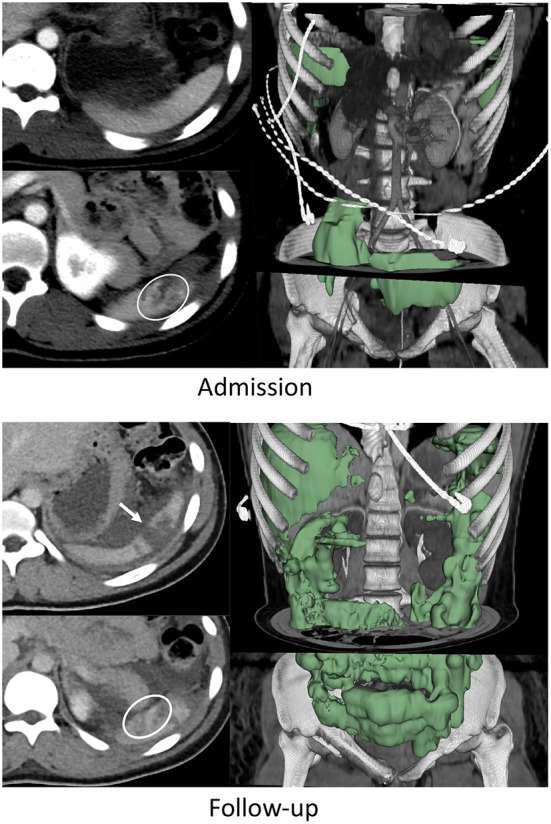
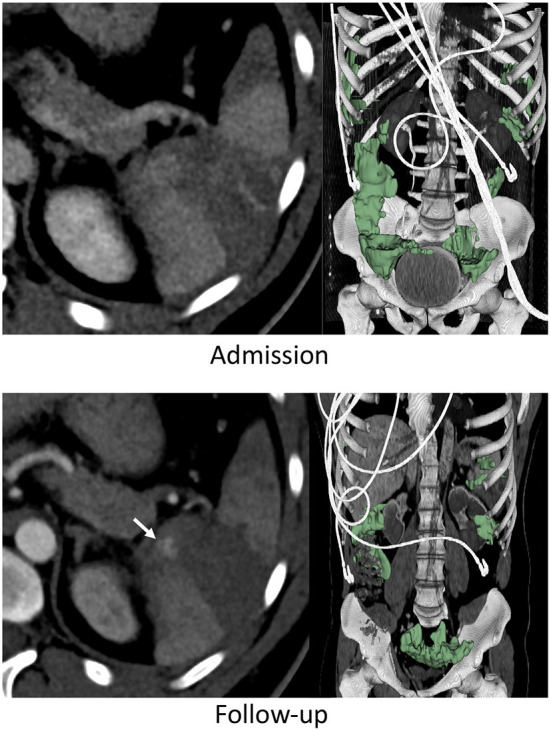
Methods: Adult patients who underwent a trial of non-operative management (NOM) with follow-up CT performed for BSI between 2017 and 2019 were included (n = 51). Six patients (12% of cohort) underwent splenectomy; 45 underwent successful splenic salvage. Voxelwise measurements of splenic laceration, hemoperitoneum, and subcapsular hematoma were derived from portal venous phase images of admission and follow-up scans using 3D slicer. Presence/absence of pseudoaneurysm on admission and follow-up CT was assessed using arterial phase images. Multivariable logistic regression was used to determine independent predictors of decision to perform splenectomy.
Results: Factors significantly associated with splenectomy in bivariate analysis incorporated in multivariate logistic regression included final hemoperitoneum volume (p = 0.003), final subcapsular hematoma volume (p = 0.001), change in subcapsular hematoma volume between scans (p = 0.09) and new/persistent pseudoaneurysm (p = 0.003). Independent predictors of splenectomy in the logistic regression were final hemoperitoneum volume (unit OR = 1.43 for each 100 mL change; 95% CI: 0.99-2.06) and new/persistent pseudoaneurysm (OR = 160.3; 95% CI: 0.91-28315.3). The AUC of the model incorporating both variables was significantly higher than AAST grading (0.91 vs. 0.59, p = 0.025). Mean combined effective dose for admission and follow up CT scans was 37.4 mSv.
Conclusion: Follow-up CT provides clinically valuable information regarding the decision to perform splenectomy in BSI patients managed non-operatively. Hemoperitoneum volume and new or persistent pseudoaneurysm at follow-up are independent predictors of splenectomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


