{"title":"Malaria Surveillance - United States, 2018.","authors":"Kimberly E Mace, Naomi W Lucchi, Kathrine R Tan","doi":"10.15585/mmwr.ss7108a1","DOIUrl":null,"url":null,"abstract":"<p><strong>Problem/condition: </strong>Malaria in humans is caused by intraerythrocytic protozoa of the genus Plasmodium. These parasites are transmitted by the bite of an infective female Anopheles species mosquito. Most malaria infections in the United States and its territories occur among persons who have traveled to regions with ongoing malaria transmission. However, among persons who have not traveled out of the country, malaria is occasionally acquired through exposure to infected blood or tissues, congenital transmission, nosocomial exposure, or local mosquitoborne transmission. Malaria surveillance in the United States and its territories provides information on its occurrence (e.g., temporal, geographic, and demographic), guides prevention and treatment recommendations for travelers and patients, and facilitates rapid transmission control measures if locally acquired cases are identified.</p><p><strong>Period covered: </strong>This report summarizes confirmed malaria cases in persons with onset of illness in 2018 and trends in previous years.</p><p><strong>Description of system: </strong>Malaria cases diagnosed by blood smear microscopy, polymerase chain reaction, or rapid diagnostic tests are reported to local and state health departments through electronic laboratory reports or by health care providers or laboratory staff members directly reporting to CDC or health departments. Case investigations are conducted by local and state health departments, and reports are transmitted to CDC through the National Malaria Surveillance System (NMSS), the National Notifiable Diseases Surveillance System (NNDSS), or direct CDC clinical consultations. CDC reference laboratories provide diagnostic assistance and conduct antimalarial drug resistance marker testing on blood specimens submitted by health care providers or local or state health departments. This report summarizes data from the integration of all cases from NMSS and NNDSS, CDC clinical consultations, and CDC reference laboratory reports.</p><p><strong>Results: </strong>CDC received reports of 1,823 confirmed malaria cases with onset of symptoms in 2018, including one cryptic case and one case acquired through a bone marrow transplant. The number of cases reported in 2018 is 15.6% fewer than in 2017. The number of cases diagnosed in the United States and its territories has been increasing since the mid-1970s; the number of cases reported in 2017 was the highest since 1972. Of the cases in 2018, a total of 1,519 (85.0%) were imported cases that originated from Africa; 1,061 (69.9%) of the cases from Africa were from West Africa, a similar proportion to what was observed in 2017. Among all cases, P. falciparum accounted for most infections (1,273 [69.8%]), followed by P. vivax (173 [9.5%]), P. ovale (95 [5.2%]), and P. malariae (48 [2.6%]). For the first time since 2008, an imported case of P. knowlesi was identified in the United States and its territories. Infections by two or more species accounted for 17 cases (<1.0%). The infecting species was not reported or was undetermined in 216 cases (11.9%). Most patients (92.6%) had symptom onset <90 days after returning to the United States or its territories from a country with malaria transmission. Of the U.S. civilian patients who reported reason for travel, 77.0% were visiting friends and relatives. Chemoprophylaxis with antimalarial medications are recommended for U.S. residents to prevent malaria while traveling in countries where it is endemic. Fewer U.S. residents with imported malaria reported taking any malaria chemoprophylaxis in 2018 (24.5%) than in 2017 (28.4%), and adherence was poor among those who took chemoprophylaxis. Among the 864 U.S. residents with malaria for whom information on chemoprophylaxis use and travel region were known, 95.0% did not adhere to or did not take a CDC-recommended chemoprophylaxis regimen. Among 683 women with malaria, 19 reported being pregnant. Of these, 11 pregnant women were U.S. residents, and one of whom reported taking chemoprophylaxis to prevent malaria but her adherence to chemoprophylaxis was not reported. Thirty-eight (2.1%) malaria cases occurred among U.S. military personnel in 2018, more than in 2017 (26 [1.2%]). Among all reported malaria cases in 2018, a total of 251 (13.8%) were classified as severe malaria illness, and seven persons died from malaria. In 2018, CDC analyzed 106 P. falciparum-positive and four P. falciparum mixed species specimens for antimalarial resistance markers (although certain loci were untestable in some specimens); identification of genetic polymorphisms associated with resistance to pyrimethamine were found in 99 (98.0%), to sulfadoxine in 49 (49.6%), to chloroquine in 50 (45.5%), and to mefloquine in two (2.0%); no specimens tested contained a marker for atovaquone or artemisinin resistance.</p><p><strong>Interpretation: </strong>The importation of malaria reflects the overall trends in global travel to and from areas where malaria is endemic, and 15.6% fewer cases were imported in 2018 compared with 2017. Of imported cases, 59.3% were among persons who had traveled from West Africa. Among U.S. civilians, visiting friends and relatives was the most common reason for travel (77.1%).</p><p><strong>Public health actions: </strong>The best way for U.S. residents to prevent malaria is to take chemoprophylaxis medication before, during, and after travel to a country where malaria is endemic. Adherence to recommended malaria prevention strategies among U.S. travelers would reduce the number of imported cases. Reported reasons for nonadherence include prematurely stopping after leaving the area where malaria was endemic, forgetting to take the medication, and experiencing a side effect. Health care providers can make travelers aware of the risks posed by malaria and incorporate education to motivate them to be adherent to chemoprophylaxis. Malaria infections can be fatal if not diagnosed and treated promptly with antimalarial medications appropriate for the patient's age, pregnancy status, medical history, the likely country of malaria acquisition, and previous use of antimalarial chemoprophylaxis. Antimalarial use for chemoprophylaxis and treatment should be determined by the CDC guidelines, which are frequently updated. In April 2019, intravenous (IV) artesunate became the first-line medication for treatment of severe malaria in the United States and its territories. Artesunate was approved by the Food and Drug Administration (FDA) in 2020 and is commercially available (Artesunate for Injection) from major U.S. drug distributors (https://amivas.com). Stocking IV artesunate locally allows for immediate treatment of severe malaria once diagnosed and provides patients with the best chance of a complete recovery and no sequelae. With commercial IV artesunate now available, CDC will discontinue distribution of non-FDA-approved IV artesunate under an investigational new drug protocol on September 30, 2022. Detailed recommendations for preventing malaria are online at https://www.cdc.gov/malaria/travelers/drugs.html. Malaria diagnosis and treatment recommendations are also available online at https://www.cdc.gov/malaria/diagnosis_treatment. Health care providers who have sought urgent infectious disease consultation and require additional assistance on diagnosis and treatment of malaria can call the Malaria Hotline 9:00 a.m.-5:00 p.m. Eastern Time, Monday-Friday, at 770-488-7788 or 855-856-4713 or after hours for urgent inquiries at 770-488-7100. Persons submitting malaria case reports (care providers, laboratories, and state and local public health officials) should provide complete information because incomplete reporting compromises case investigations and public health efforts to prevent future infections and examine trends in malaria cases. Molecular surveillance of antimalarial drug resistance markers enables CDC to track, guide treatment, and manage drug resistance in malaria parasites both domestically and globally. A greater proportion of specimens from domestic malaria cases are needed to improve the completeness of antimalarial drug resistance analysis; therefore, CDC requests that blood specimens be submitted for any case of malaria diagnosed in the United States and its territories.</p>","PeriodicalId":48549,"journal":{"name":"Mmwr Surveillance Summaries","volume":"71 8","pages":"1-35"},"PeriodicalIF":49.8000,"publicationDate":"2022-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9470224/pdf/","citationCount":"16","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mmwr Surveillance Summaries","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.15585/mmwr.ss7108a1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 16
Abstract
Problem/condition: Malaria in humans is caused by intraerythrocytic protozoa of the genus Plasmodium. These parasites are transmitted by the bite of an infective female Anopheles species mosquito. Most malaria infections in the United States and its territories occur among persons who have traveled to regions with ongoing malaria transmission. However, among persons who have not traveled out of the country, malaria is occasionally acquired through exposure to infected blood or tissues, congenital transmission, nosocomial exposure, or local mosquitoborne transmission. Malaria surveillance in the United States and its territories provides information on its occurrence (e.g., temporal, geographic, and demographic), guides prevention and treatment recommendations for travelers and patients, and facilitates rapid transmission control measures if locally acquired cases are identified.
Period covered: This report summarizes confirmed malaria cases in persons with onset of illness in 2018 and trends in previous years.
Description of system: Malaria cases diagnosed by blood smear microscopy, polymerase chain reaction, or rapid diagnostic tests are reported to local and state health departments through electronic laboratory reports or by health care providers or laboratory staff members directly reporting to CDC or health departments. Case investigations are conducted by local and state health departments, and reports are transmitted to CDC through the National Malaria Surveillance System (NMSS), the National Notifiable Diseases Surveillance System (NNDSS), or direct CDC clinical consultations. CDC reference laboratories provide diagnostic assistance and conduct antimalarial drug resistance marker testing on blood specimens submitted by health care providers or local or state health departments. This report summarizes data from the integration of all cases from NMSS and NNDSS, CDC clinical consultations, and CDC reference laboratory reports.
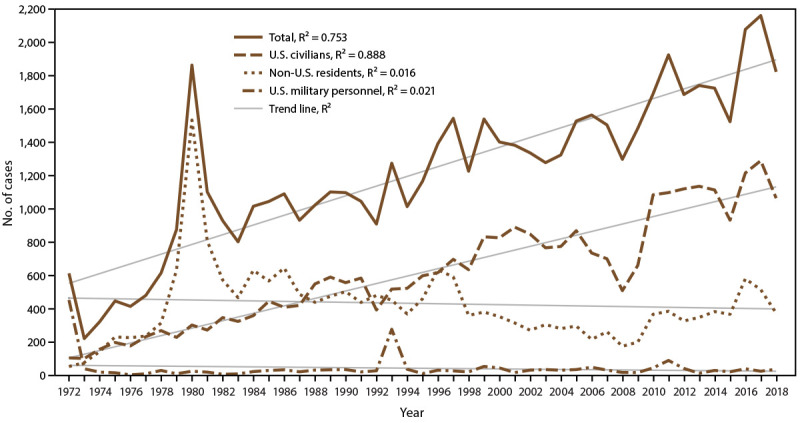
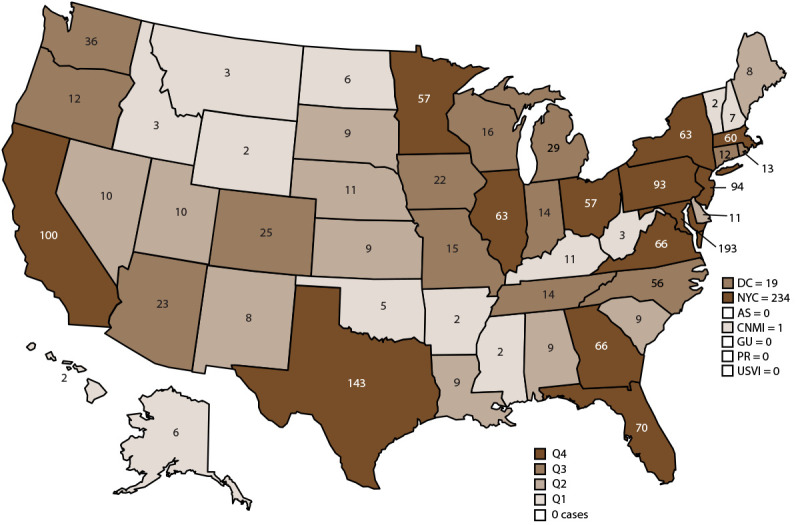
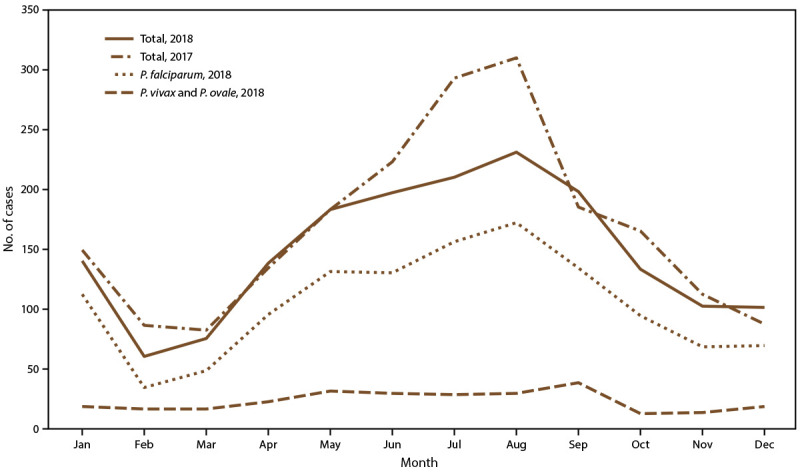
Results: CDC received reports of 1,823 confirmed malaria cases with onset of symptoms in 2018, including one cryptic case and one case acquired through a bone marrow transplant. The number of cases reported in 2018 is 15.6% fewer than in 2017. The number of cases diagnosed in the United States and its territories has been increasing since the mid-1970s; the number of cases reported in 2017 was the highest since 1972. Of the cases in 2018, a total of 1,519 (85.0%) were imported cases that originated from Africa; 1,061 (69.9%) of the cases from Africa were from West Africa, a similar proportion to what was observed in 2017. Among all cases, P. falciparum accounted for most infections (1,273 [69.8%]), followed by P. vivax (173 [9.5%]), P. ovale (95 [5.2%]), and P. malariae (48 [2.6%]). For the first time since 2008, an imported case of P. knowlesi was identified in the United States and its territories. Infections by two or more species accounted for 17 cases (<1.0%). The infecting species was not reported or was undetermined in 216 cases (11.9%). Most patients (92.6%) had symptom onset <90 days after returning to the United States or its territories from a country with malaria transmission. Of the U.S. civilian patients who reported reason for travel, 77.0% were visiting friends and relatives. Chemoprophylaxis with antimalarial medications are recommended for U.S. residents to prevent malaria while traveling in countries where it is endemic. Fewer U.S. residents with imported malaria reported taking any malaria chemoprophylaxis in 2018 (24.5%) than in 2017 (28.4%), and adherence was poor among those who took chemoprophylaxis. Among the 864 U.S. residents with malaria for whom information on chemoprophylaxis use and travel region were known, 95.0% did not adhere to or did not take a CDC-recommended chemoprophylaxis regimen. Among 683 women with malaria, 19 reported being pregnant. Of these, 11 pregnant women were U.S. residents, and one of whom reported taking chemoprophylaxis to prevent malaria but her adherence to chemoprophylaxis was not reported. Thirty-eight (2.1%) malaria cases occurred among U.S. military personnel in 2018, more than in 2017 (26 [1.2%]). Among all reported malaria cases in 2018, a total of 251 (13.8%) were classified as severe malaria illness, and seven persons died from malaria. In 2018, CDC analyzed 106 P. falciparum-positive and four P. falciparum mixed species specimens for antimalarial resistance markers (although certain loci were untestable in some specimens); identification of genetic polymorphisms associated with resistance to pyrimethamine were found in 99 (98.0%), to sulfadoxine in 49 (49.6%), to chloroquine in 50 (45.5%), and to mefloquine in two (2.0%); no specimens tested contained a marker for atovaquone or artemisinin resistance.
Interpretation: The importation of malaria reflects the overall trends in global travel to and from areas where malaria is endemic, and 15.6% fewer cases were imported in 2018 compared with 2017. Of imported cases, 59.3% were among persons who had traveled from West Africa. Among U.S. civilians, visiting friends and relatives was the most common reason for travel (77.1%).
Public health actions: The best way for U.S. residents to prevent malaria is to take chemoprophylaxis medication before, during, and after travel to a country where malaria is endemic. Adherence to recommended malaria prevention strategies among U.S. travelers would reduce the number of imported cases. Reported reasons for nonadherence include prematurely stopping after leaving the area where malaria was endemic, forgetting to take the medication, and experiencing a side effect. Health care providers can make travelers aware of the risks posed by malaria and incorporate education to motivate them to be adherent to chemoprophylaxis. Malaria infections can be fatal if not diagnosed and treated promptly with antimalarial medications appropriate for the patient's age, pregnancy status, medical history, the likely country of malaria acquisition, and previous use of antimalarial chemoprophylaxis. Antimalarial use for chemoprophylaxis and treatment should be determined by the CDC guidelines, which are frequently updated. In April 2019, intravenous (IV) artesunate became the first-line medication for treatment of severe malaria in the United States and its territories. Artesunate was approved by the Food and Drug Administration (FDA) in 2020 and is commercially available (Artesunate for Injection) from major U.S. drug distributors (https://amivas.com). Stocking IV artesunate locally allows for immediate treatment of severe malaria once diagnosed and provides patients with the best chance of a complete recovery and no sequelae. With commercial IV artesunate now available, CDC will discontinue distribution of non-FDA-approved IV artesunate under an investigational new drug protocol on September 30, 2022. Detailed recommendations for preventing malaria are online at https://www.cdc.gov/malaria/travelers/drugs.html. Malaria diagnosis and treatment recommendations are also available online at https://www.cdc.gov/malaria/diagnosis_treatment. Health care providers who have sought urgent infectious disease consultation and require additional assistance on diagnosis and treatment of malaria can call the Malaria Hotline 9:00 a.m.-5:00 p.m. Eastern Time, Monday-Friday, at 770-488-7788 or 855-856-4713 or after hours for urgent inquiries at 770-488-7100. Persons submitting malaria case reports (care providers, laboratories, and state and local public health officials) should provide complete information because incomplete reporting compromises case investigations and public health efforts to prevent future infections and examine trends in malaria cases. Molecular surveillance of antimalarial drug resistance markers enables CDC to track, guide treatment, and manage drug resistance in malaria parasites both domestically and globally. A greater proportion of specimens from domestic malaria cases are needed to improve the completeness of antimalarial drug resistance analysis; therefore, CDC requests that blood specimens be submitted for any case of malaria diagnosed in the United States and its territories.
期刊介绍:
The Morbidity and Mortality Weekly Report (MMWR) Series, produced by the Centers for Disease Control and Prevention (CDC), is commonly referred to as "the voice of CDC." Serving as the primary outlet for timely, reliable, authoritative, accurate, objective, and practical public health information and recommendations, the MMWR is a crucial publication. Its readership primarily includes physicians, nurses, public health practitioners, epidemiologists, scientists, researchers, educators, and laboratorians.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


