Rachael Oxman , Andrea H. Roe , Jagdeesh Ullal , Melissa S. Putman
{"title":"Gestational and pregestational diabetes in pregnant women with cystic fibrosis","authors":"Rachael Oxman , Andrea H. Roe , Jagdeesh Ullal , Melissa S. Putman","doi":"10.1016/j.jcte.2021.100289","DOIUrl":null,"url":null,"abstract":"<div><p>As cystic fibrosis transmembrane regulator (CFTR) modulator therapies offer greater longevity and improved health quality, women living with cystic fibrosis (CF) are increasingly pursuing pregnancy. Maternal risks for pregnant women with CF largely depend on a woman’s baseline pulmonary and pancreatic function, and the majority of CF pregnancies will successfully end in live births.</p><p>Diabetes, either gestational or pre-existing cystic fibrosis-related diabetes (CFRD), is highly prevalent in women with CF, affecting 18 to 62% of pregnancies in recent CF center reports. In addition to the rising incidence of CFRD with age, gestational diabetes is also more common in women with CF due to lower insulin secretion, higher insulin resistance, and increased hepatic glucose production as compared to pregnant women without CF. Diabetes occurring during pregnancy has important implications for maternal and fetal health. It is well established in women without CF that glycemic control is directly associated with risks of fetal malformation, neonatal-perinatal mortality, cesarean delivery and need for neonatal intensive care. Small studies in women with CF suggest that pregnancies affected by diabetes have an increased risk of preterm delivery, lower gestational age, and lower fetal birth weight compared to those without diabetes.</p><p>Women with CF preparing for pregnancy should be counseled on the risks of diabetes and should undergo routine screening for CFRD with oral glucose tolerance testing (OGTT) if not already completed in the past six months. Glycemic control in those with pre-gestational CFRD should be optimized prior to conception. Insulin is preferred for the management of diabetes in pregnant women with CF via multiple daily injections or insulin pump therapy, and continuous glucose monitors (CGM) can be useful in mitigating hypoglycemia risks. Women with CF face many unique challenges impacting diabetes care during pregnancy and would benefit from support by a multidisciplinary care team, including nutrition and endocrinology, to ensure healthy pregnancies.</p></div>","PeriodicalId":46328,"journal":{"name":"Journal of Clinical and Translational Endocrinology","volume":"27 ","pages":"Article 100289"},"PeriodicalIF":4.2000,"publicationDate":"2022-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fb/64/main.PMC8693285.pdf","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Translational Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2214623721000417","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 7
Abstract
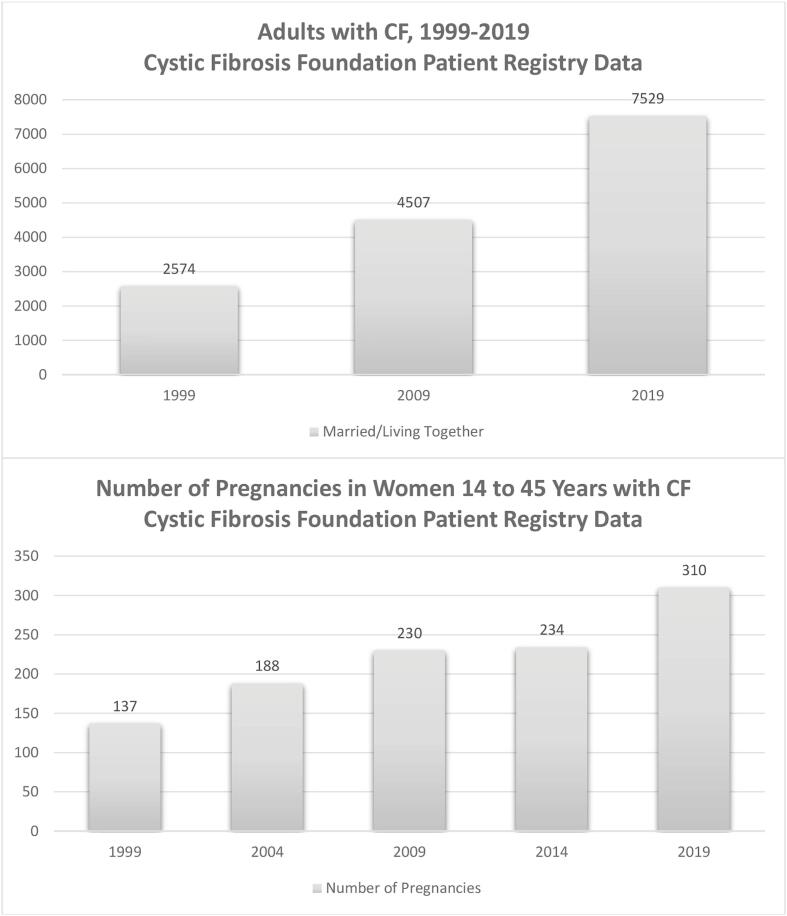
As cystic fibrosis transmembrane regulator (CFTR) modulator therapies offer greater longevity and improved health quality, women living with cystic fibrosis (CF) are increasingly pursuing pregnancy. Maternal risks for pregnant women with CF largely depend on a woman’s baseline pulmonary and pancreatic function, and the majority of CF pregnancies will successfully end in live births.
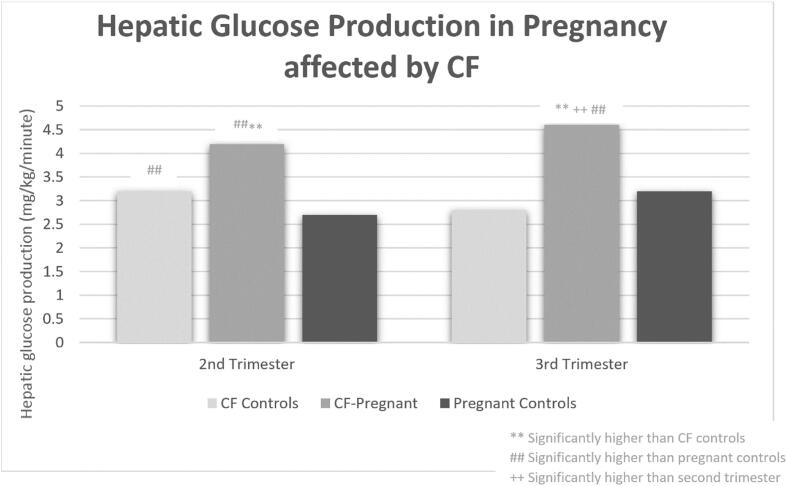
Diabetes, either gestational or pre-existing cystic fibrosis-related diabetes (CFRD), is highly prevalent in women with CF, affecting 18 to 62% of pregnancies in recent CF center reports. In addition to the rising incidence of CFRD with age, gestational diabetes is also more common in women with CF due to lower insulin secretion, higher insulin resistance, and increased hepatic glucose production as compared to pregnant women without CF. Diabetes occurring during pregnancy has important implications for maternal and fetal health. It is well established in women without CF that glycemic control is directly associated with risks of fetal malformation, neonatal-perinatal mortality, cesarean delivery and need for neonatal intensive care. Small studies in women with CF suggest that pregnancies affected by diabetes have an increased risk of preterm delivery, lower gestational age, and lower fetal birth weight compared to those without diabetes.
Women with CF preparing for pregnancy should be counseled on the risks of diabetes and should undergo routine screening for CFRD with oral glucose tolerance testing (OGTT) if not already completed in the past six months. Glycemic control in those with pre-gestational CFRD should be optimized prior to conception. Insulin is preferred for the management of diabetes in pregnant women with CF via multiple daily injections or insulin pump therapy, and continuous glucose monitors (CGM) can be useful in mitigating hypoglycemia risks. Women with CF face many unique challenges impacting diabetes care during pregnancy and would benefit from support by a multidisciplinary care team, including nutrition and endocrinology, to ensure healthy pregnancies.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


