Adam B Smith, Andria Hanbury, Jennifer A Whitty, Igor Beitia Ortiz de Zarate, Florence Hammes, Gérard de Pouvourville, Katharina Buesch
{"title":"A Discrete Choice Experiment to Derive Health Utilities for Aromatic L-Amino Acid Decarboxylase (AADC) Deficiency in France.","authors":"Adam B Smith, Andria Hanbury, Jennifer A Whitty, Igor Beitia Ortiz de Zarate, Florence Hammes, Gérard de Pouvourville, Katharina Buesch","doi":"10.2147/PROM.S332519","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Cost-effectiveness evaluations of interventions require health utility data. However, in medical conditions, such as aromatic L-amino acid decarboxylase (AADC) deficiency, this presents problems due to the rarity of the disease. The study aim therefore was to employ a discrete choice experiment (DCE) to generate health utilities for AADC deficiency.</p><p><strong>Methods: </strong>A previous literature review, clinician and parent interviews had identified six key AADC deficiency attributes: mobility, muscle weakness, oculogyric crises (OCG), feeding ability, cognitive impairment and screaming. A representative sample of the French general population was recruited. Participants rated 5 health state vignettes describing AADC deficiency using time-trade-off (TTO) and standard gamble (SG). Additionally, participants rated the worst health state using the Health Utility Index version 3 (HUI3). Subsequently, participants completed DCE 11 choice sets. Indirect DCE part-worth utilities were converted to health utilities using the anchors from the TTO, SG and HUI3.</p><p><strong>Results: </strong>The DCE was completed online by 1001 participants (50.9% female; mean age 45.7 years). Most participants (596, 59.5%) provided consistent responses to the repeated choice task. Five models were evaluated, and one preference reversal (\"head control\"/\"sitting unaided\") was identified in all models. The rescaled utilities ranged from 0.3891 to 0.5577 (difference of 0.17 utilities) for TTO anchors corresponding to the worst (633233) and best (111111) health states. Health utilities ranged from 0.5534 to 0.7093 for the SG anchors. The disutility associated with a transition from \"no problems walking\" to \"bedridden\" was -0.0533, whereas disutility of moving from \"constant screaming\" relative to \"no screaming\" was -0.0248. The disutility associated with daily OCG was -0.0167. Disutilities for the other attributes were small although there were exceptions.</p><p><strong>Conclusion: </strong>A DCE was used to derive health utilities for AADC deficiency. These health utilities will subsequently be used in an economic model evaluating an AADC deficiency intervention.</p>","PeriodicalId":19747,"journal":{"name":"Patient Related Outcome Measures","volume":" ","pages":"21-30"},"PeriodicalIF":1.8000,"publicationDate":"2022-01-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f6/b8/prom-13-21.PMC8800863.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Patient Related Outcome Measures","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/PROM.S332519","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Cost-effectiveness evaluations of interventions require health utility data. However, in medical conditions, such as aromatic L-amino acid decarboxylase (AADC) deficiency, this presents problems due to the rarity of the disease. The study aim therefore was to employ a discrete choice experiment (DCE) to generate health utilities for AADC deficiency.
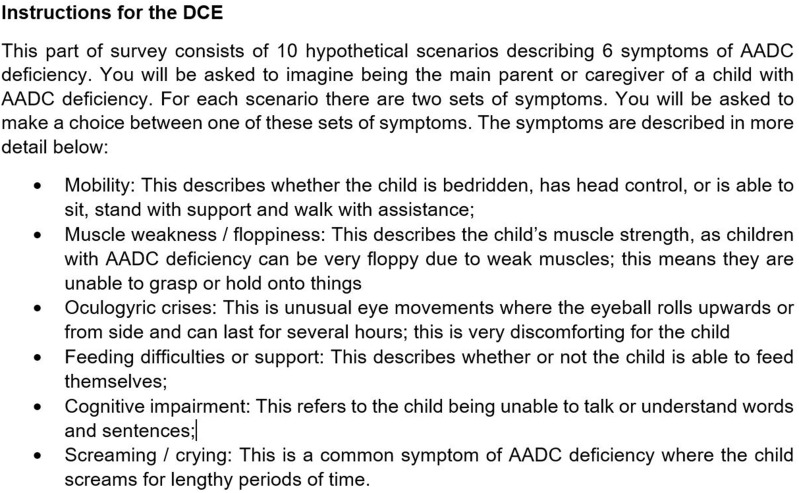
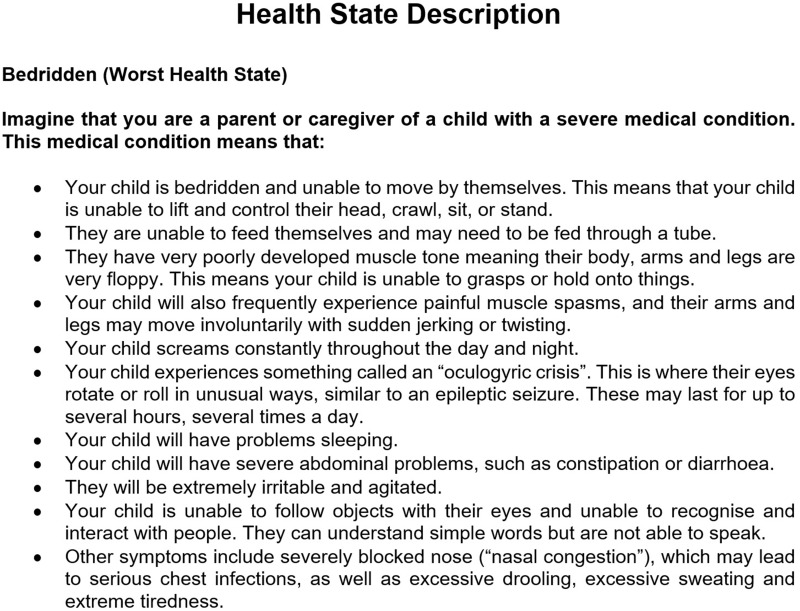
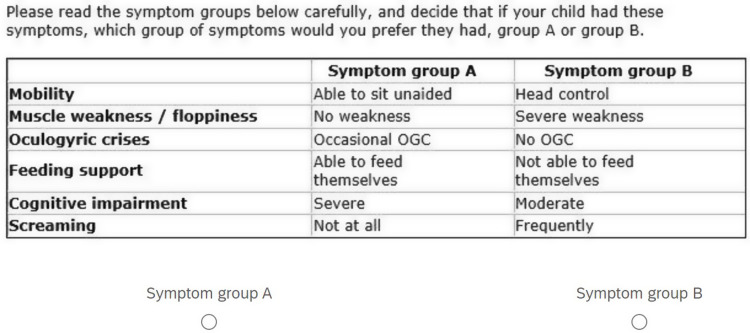
Methods: A previous literature review, clinician and parent interviews had identified six key AADC deficiency attributes: mobility, muscle weakness, oculogyric crises (OCG), feeding ability, cognitive impairment and screaming. A representative sample of the French general population was recruited. Participants rated 5 health state vignettes describing AADC deficiency using time-trade-off (TTO) and standard gamble (SG). Additionally, participants rated the worst health state using the Health Utility Index version 3 (HUI3). Subsequently, participants completed DCE 11 choice sets. Indirect DCE part-worth utilities were converted to health utilities using the anchors from the TTO, SG and HUI3.
Results: The DCE was completed online by 1001 participants (50.9% female; mean age 45.7 years). Most participants (596, 59.5%) provided consistent responses to the repeated choice task. Five models were evaluated, and one preference reversal ("head control"/"sitting unaided") was identified in all models. The rescaled utilities ranged from 0.3891 to 0.5577 (difference of 0.17 utilities) for TTO anchors corresponding to the worst (633233) and best (111111) health states. Health utilities ranged from 0.5534 to 0.7093 for the SG anchors. The disutility associated with a transition from "no problems walking" to "bedridden" was -0.0533, whereas disutility of moving from "constant screaming" relative to "no screaming" was -0.0248. The disutility associated with daily OCG was -0.0167. Disutilities for the other attributes were small although there were exceptions.
Conclusion: A DCE was used to derive health utilities for AADC deficiency. These health utilities will subsequently be used in an economic model evaluating an AADC deficiency intervention.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


