The Value of a Systematic Protocol Using Endobronchial Ultrasound and Endoscopic Ultrasound in Staging of Lung Cancer for Patients with Imaging iN0-N1 Disease.
Rosa Cordovilla, Marco López-Zubizarreta, Antonio Velasco, Alberto Álvarez, Marta Rodríguez, Asunción Gómez, Miguel Ángel Hernández-Mezquita, Miguel Iglesias
{"title":"The Value of a Systematic Protocol Using Endobronchial Ultrasound and Endoscopic Ultrasound in Staging of Lung Cancer for Patients with Imaging iN0-N1 Disease.","authors":"Rosa Cordovilla, Marco López-Zubizarreta, Antonio Velasco, Alberto Álvarez, Marta Rodríguez, Asunción Gómez, Miguel Ángel Hernández-Mezquita, Miguel Iglesias","doi":"10.1159/000519034","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>We hypothesize that systematic, combined, and multidisciplinary study of the mediastinum (endobronchial ultrasound [EBUS] and endoscopic ultrasound [EUS]) in patients with NSCLC with radiologically normal mediastinum improves the results of mediastinal staging obtained with EBUS alone.</p><p><strong>Material and methods: </strong>A retrospective study of the prospective database collected on the patients with NSCLC with a radiologically normal mediastinum and an indication for systematic staging with EBUS and EUS. EBUS staging was followed by EUS in patients in which the results from the pathological analysis of EBUS were negative.</p><p><strong>Results: </strong>Forty-five patients were included in the analysis. The combination of EBUS followed by EUS provided better results than EBUS alone: sensitivity (S) 95% versus 80%, negative predictive value (NPV) 96.15% versus 86.21%, negative likelihood ratio 0.05 versus 0.20, and post-test probability 3.8% versus 13.8%. This represents an increase in S (15%), the validity index (6.6%), and NPV (9.9%) compared to EBUS alone. There were 4 false negatives (FNs) (8.8%) with the EBUS test alone. After adding EUS, 3 more cases were positive (6.6%) and only 1 FN (2.2%).</p><p><strong>Conclusions: </strong>In patients with NSCLC and a radiographically normal mediastinum, a systematic and combined staging with EBUS and EUS show higher sensitivity in the detection of mediastinal metastasis than with the use of EBUS alone. The high accuracy of the test means that the use of mediastinoscopy is not necessary to confirm the results in these patients. Since the availability of EUS is low, it may be advisable for the interventional pulmonologist to receive training in EUS-b.</p>","PeriodicalId":9075,"journal":{"name":"Biomedicine Hub","volume":"6 3","pages":"92-101"},"PeriodicalIF":0.0000,"publicationDate":"2021-10-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/19/9a/bmh-0006-0092.PMC8613614.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomedicine Hub","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000519034","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: We hypothesize that systematic, combined, and multidisciplinary study of the mediastinum (endobronchial ultrasound [EBUS] and endoscopic ultrasound [EUS]) in patients with NSCLC with radiologically normal mediastinum improves the results of mediastinal staging obtained with EBUS alone.
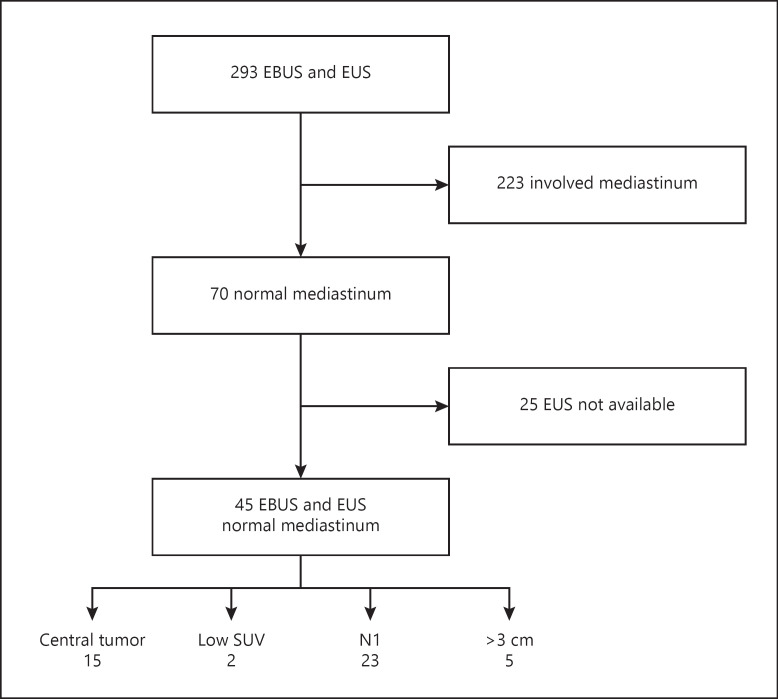
Material and methods: A retrospective study of the prospective database collected on the patients with NSCLC with a radiologically normal mediastinum and an indication for systematic staging with EBUS and EUS. EBUS staging was followed by EUS in patients in which the results from the pathological analysis of EBUS were negative.
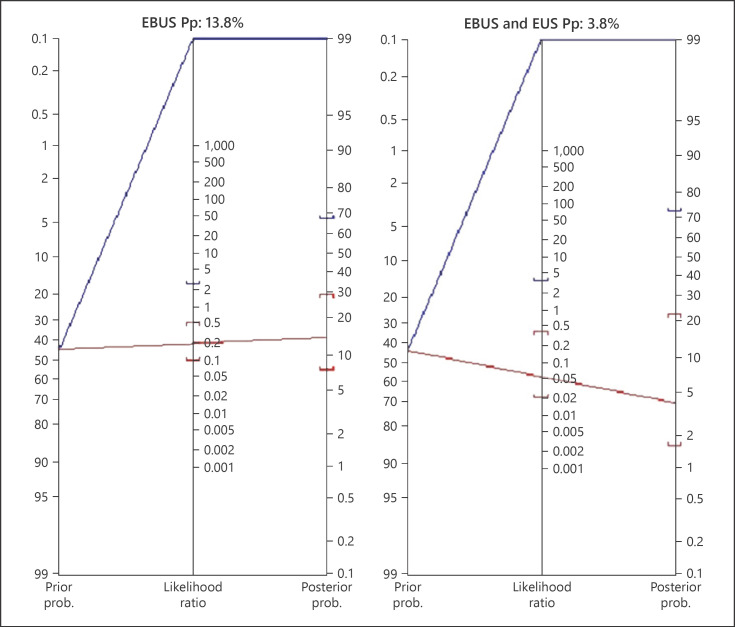
Results: Forty-five patients were included in the analysis. The combination of EBUS followed by EUS provided better results than EBUS alone: sensitivity (S) 95% versus 80%, negative predictive value (NPV) 96.15% versus 86.21%, negative likelihood ratio 0.05 versus 0.20, and post-test probability 3.8% versus 13.8%. This represents an increase in S (15%), the validity index (6.6%), and NPV (9.9%) compared to EBUS alone. There were 4 false negatives (FNs) (8.8%) with the EBUS test alone. After adding EUS, 3 more cases were positive (6.6%) and only 1 FN (2.2%).
Conclusions: In patients with NSCLC and a radiographically normal mediastinum, a systematic and combined staging with EBUS and EUS show higher sensitivity in the detection of mediastinal metastasis than with the use of EBUS alone. The high accuracy of the test means that the use of mediastinoscopy is not necessary to confirm the results in these patients. Since the availability of EUS is low, it may be advisable for the interventional pulmonologist to receive training in EUS-b.
我们假设系统、联合和多学科的研究(支气管超声[EBUS]和内镜超声[EUS])对放射学上正常的NSCLC纵隔患者的纵隔分期可以改善单独使用EBUS获得的纵隔分期结果。材料和方法:回顾性研究收集的纵隔放射学正常的NSCLC患者的前瞻性数据库,并采用EBUS和EUS进行系统分期。病理分析结果为阴性的患者进行EBUS分期并进行EUS检查。结果:45例患者纳入分析。EBUS联合EUS优于单独EBUS:敏感性(S) 95% vs 80%,阴性预测值(NPV) 96.15% vs 86.21%,阴性似然比0.05 vs 0.20,验后概率3.8% vs 13.8%。与单独的EBUS相比,这代表了S(15%)、有效性指数(6.6%)和NPV(9.9%)的增加。单独使用EBUS检测出现4例假阴性(FNs),占8.8%。加EUS后阳性3例(6.6%),FN仅1例(2.2%)。结论:在影像学正常的非小细胞肺癌纵隔患者中,与单独使用EBUS相比,系统和联合分期EBUS和EUS在检测纵隔转移方面具有更高的敏感性。测试的高准确性意味着在这些患者中不需要使用纵隔镜检查来确认结果。由于EUS的可用性较低,介入肺科医生接受EUS-b培训可能是可取的。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


