John Nicolet, Yolanda Mueller, Paola Paruta, Julien Boucher, Nicolas Senn
{"title":"What is the carbon footprint of primary care practices? A retrospective life-cycle analysis in Switzerland.","authors":"John Nicolet, Yolanda Mueller, Paola Paruta, Julien Boucher, Nicolas Senn","doi":"10.1186/s12940-021-00814-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The medical field causes significant environmental impact. Reduction of the primary care practice carbon footprint could contribute to decreasing global carbon emissions. This study aims to quantify the average carbon footprint of a primary care consultation, describe differences between primary care practices (best, worst and average performing) in western Switzerland and identify opportunities for mitigation.</p><p><strong>Methods: </strong>We conducted a retrospective carbon footprint analysis of ten private practices over the year 2018. We used life-cycle analysis to estimate carbon emissions of each sector, from manufacture to disposal, expressing results as CO<sub>2</sub> equivalents per average consultation and practice. We then modelled an average and theoretical best- case and worst-case practices. Collected data included invoices, medical and furniture inventories, heating and power supply, staff and patient transport, laboratory analyses (in/out-house) waste quantities and management costs.</p><p><strong>Results: </strong>An average medical consultation generated 4.8 kg of CO<sub>2</sub>eq and overall, an average practice produced 30 tons of CO<sub>2</sub>eq per year, with 45.7% for staff and patient transport and 29.8% for heating. Medical consumables produced 5.5% of CO<sub>2</sub>eq emissions, while in-house laboratory and X-rays contributed less than 1% each. Emergency analyses requiring courier transport caused 5.8% of all emissions. Support activities generated 82.6% of the total CO<sub>2</sub>eq. Simulation of best- and worst-case scenarios resulted in a ten-fold variation in CO<sub>2</sub>eq emissions.</p><p><strong>Conclusion: </strong>Optimizing structural and organisational aspects of practice work could have a major impact on the carbon footprint of primary care practices without large-scale changes in medical activities.</p>","PeriodicalId":520610,"journal":{"name":"Environmental health : a global access science source","volume":" ","pages":"3"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8723904/pdf/","citationCount":"17","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Environmental health : a global access science source","FirstCategoryId":"93","ListUrlMain":"https://doi.org/10.1186/s12940-021-00814-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 17
Abstract
Background: The medical field causes significant environmental impact. Reduction of the primary care practice carbon footprint could contribute to decreasing global carbon emissions. This study aims to quantify the average carbon footprint of a primary care consultation, describe differences between primary care practices (best, worst and average performing) in western Switzerland and identify opportunities for mitigation.
Methods: We conducted a retrospective carbon footprint analysis of ten private practices over the year 2018. We used life-cycle analysis to estimate carbon emissions of each sector, from manufacture to disposal, expressing results as CO2 equivalents per average consultation and practice. We then modelled an average and theoretical best- case and worst-case practices. Collected data included invoices, medical and furniture inventories, heating and power supply, staff and patient transport, laboratory analyses (in/out-house) waste quantities and management costs.
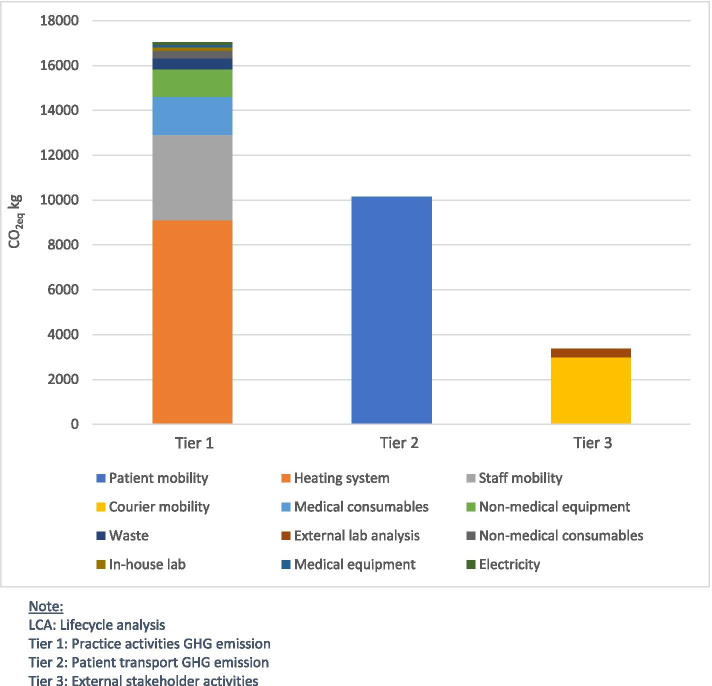
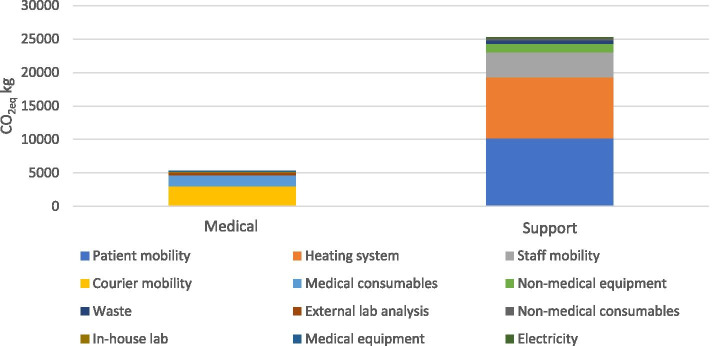
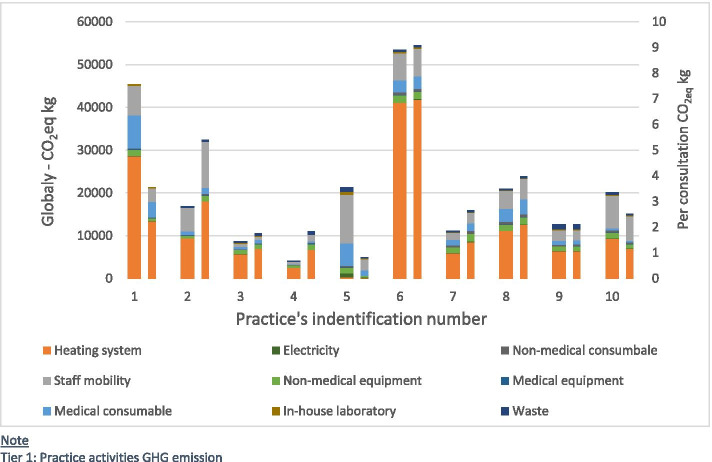
Results: An average medical consultation generated 4.8 kg of CO2eq and overall, an average practice produced 30 tons of CO2eq per year, with 45.7% for staff and patient transport and 29.8% for heating. Medical consumables produced 5.5% of CO2eq emissions, while in-house laboratory and X-rays contributed less than 1% each. Emergency analyses requiring courier transport caused 5.8% of all emissions. Support activities generated 82.6% of the total CO2eq. Simulation of best- and worst-case scenarios resulted in a ten-fold variation in CO2eq emissions.
Conclusion: Optimizing structural and organisational aspects of practice work could have a major impact on the carbon footprint of primary care practices without large-scale changes in medical activities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


