Timothy Eden, Shane McAuliffe, Dominic Crocombe, Jonathan Neville, Sumantra Ray
{"title":"Nutritional parameters and outcomes in patients admitted to intensive care with COVID-19: a retrospective single-centre service evaluation.","authors":"Timothy Eden, Shane McAuliffe, Dominic Crocombe, Jonathan Neville, Sumantra Ray","doi":"10.1136/bmjnph-2021-000270","DOIUrl":null,"url":null,"abstract":"<p><p>COVID-19 is an inflammatory syndrome caused by novel coronavirus SARS-CoV-2. Symptoms range from mild infection to severe acute respiratory distress syndrome (ARDS) requiring ventilation and intensive care. At the time of data collection, UK cases were around 300 000 with a fatality rate of 13% necessitating over 10 000 critical care admissions; now there have been over 4 million cases. Nutrition is important to immune function and influences metabolic risk factors such as obesity and glycaemic control, as well as recovery from acute illnesses. Poor nutritional status is associated with worse outcomes in ARDS and viral infections, yet limited research has assessed pre-morbid nutritional status and outcomes in patients critically unwell with COVID-19.</p><p><strong>Objectives: </strong>Investigate the effect of body mass index (BMI), glycaemic control and vitamin D status on outcomes in adult patients with COVID-19 admitted to an intensive care unit (ICU).</p><p><strong>Methods: </strong>Retrospective review of all patients admitted to a central London ICU between March and May 2020 with confirmed COVID-19. Electronic patient records data were analysed for patient demographics; comorbidities; admission BMI; and serum vitamin D, zinc, selenium and haemoglobin A1c (HbA1c) concentrations. Serum vitamin D and HbA1c were measured on admission, or within 1 month of admission to ICU. Primary outcome of interest was mortality. Secondary outcomes included time intubated, ICU stay duration and ICU-related morbidity.</p><p><strong>Results: </strong>Seventy-two patients; 54 (75%) men, mean age 57.1 (±9.8) years, were included. Overall, mortality was 24 (33%). No significant association with mortality was observed across BMI categories. In the survival arm admission, HbA1c (mmol/mol) was lower, 50.2 vs 60.8, but this was not statistically significant. Vitamin D status did not significantly associate with mortality (p=0.131). However, 32% of patients with low vitamin D (<25 IU/L) died, compared with 13% of patients with vitamin D levels >26 IU/L. Serum zinc and selenium, and vitamin B<sub>12</sub> and folate levels were measured in 46% and 26% of patients, respectively.</p><p><strong>Discussion/conclusion: </strong>Increased adiposity and deranged glucose homeostasis may potentially increase risk of COVID-19 infection and severity, possibly relating to impaired lung and metabolic function, increased proinflammatory and prothrombotic mechanisms. Vitamin D deficiency may also associate with poorer outcomes and mortality, supporting a possible role of vitamin D in immune function specific to pulmonary inflammation and COVID-19 pathophysiology. There are plausible associations between raised BMI, glycaemic control, vitamin D status and poor prognosis, as seen in wider studies; however, in this service evaluation audit during the first wave of the pandemic in the UK, with a limited data set available for this analysis, the associations did not reach statistical significance. Further research is needed into specific nutritional markers influencing critical care admissions with COVID-19.</p>","PeriodicalId":3,"journal":{"name":"ACS Applied Electronic Materials","volume":" ","pages":"416-424"},"PeriodicalIF":4.7000,"publicationDate":"2021-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1136/bmjnph-2021-000270","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Electronic Materials","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjnph-2021-000270","RegionNum":3,"RegionCategory":"材料科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"ENGINEERING, ELECTRICAL & ELECTRONIC","Score":null,"Total":0}
引用次数: 4
Abstract
COVID-19 is an inflammatory syndrome caused by novel coronavirus SARS-CoV-2. Symptoms range from mild infection to severe acute respiratory distress syndrome (ARDS) requiring ventilation and intensive care. At the time of data collection, UK cases were around 300 000 with a fatality rate of 13% necessitating over 10 000 critical care admissions; now there have been over 4 million cases. Nutrition is important to immune function and influences metabolic risk factors such as obesity and glycaemic control, as well as recovery from acute illnesses. Poor nutritional status is associated with worse outcomes in ARDS and viral infections, yet limited research has assessed pre-morbid nutritional status and outcomes in patients critically unwell with COVID-19.
Objectives: Investigate the effect of body mass index (BMI), glycaemic control and vitamin D status on outcomes in adult patients with COVID-19 admitted to an intensive care unit (ICU).
Methods: Retrospective review of all patients admitted to a central London ICU between March and May 2020 with confirmed COVID-19. Electronic patient records data were analysed for patient demographics; comorbidities; admission BMI; and serum vitamin D, zinc, selenium and haemoglobin A1c (HbA1c) concentrations. Serum vitamin D and HbA1c were measured on admission, or within 1 month of admission to ICU. Primary outcome of interest was mortality. Secondary outcomes included time intubated, ICU stay duration and ICU-related morbidity.
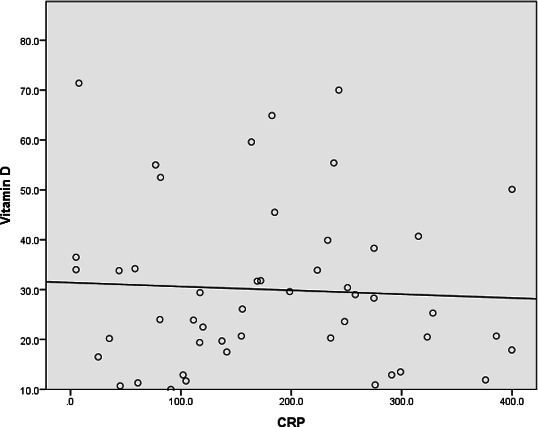
Results: Seventy-two patients; 54 (75%) men, mean age 57.1 (±9.8) years, were included. Overall, mortality was 24 (33%). No significant association with mortality was observed across BMI categories. In the survival arm admission, HbA1c (mmol/mol) was lower, 50.2 vs 60.8, but this was not statistically significant. Vitamin D status did not significantly associate with mortality (p=0.131). However, 32% of patients with low vitamin D (<25 IU/L) died, compared with 13% of patients with vitamin D levels >26 IU/L. Serum zinc and selenium, and vitamin B12 and folate levels were measured in 46% and 26% of patients, respectively.
Discussion/conclusion: Increased adiposity and deranged glucose homeostasis may potentially increase risk of COVID-19 infection and severity, possibly relating to impaired lung and metabolic function, increased proinflammatory and prothrombotic mechanisms. Vitamin D deficiency may also associate with poorer outcomes and mortality, supporting a possible role of vitamin D in immune function specific to pulmonary inflammation and COVID-19 pathophysiology. There are plausible associations between raised BMI, glycaemic control, vitamin D status and poor prognosis, as seen in wider studies; however, in this service evaluation audit during the first wave of the pandemic in the UK, with a limited data set available for this analysis, the associations did not reach statistical significance. Further research is needed into specific nutritional markers influencing critical care admissions with COVID-19.
期刊介绍:
ACS Applied Electronic Materials is an interdisciplinary journal publishing original research covering all aspects of electronic materials. The journal is devoted to reports of new and original experimental and theoretical research of an applied nature that integrate knowledge in the areas of materials science, engineering, optics, physics, and chemistry into important applications of electronic materials. Sample research topics that span the journal's scope are inorganic, organic, ionic and polymeric materials with properties that include conducting, semiconducting, superconducting, insulating, dielectric, magnetic, optoelectronic, piezoelectric, ferroelectric and thermoelectric.
Indexed/Abstracted:
Web of Science SCIE
Scopus
CAS
INSPEC
Portico
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


