A quality improvement initiative to successfully reduce the frequency of hypoglycemia during treatment of hyperglycemic crises at an academic safety-net hospital: Insights and results
Katherine L. Modzelewski, Ariana Cannavo , Kathryn L. Fantasia, Sira Korpaisarn , Sara M. Alexanian
{"title":"A quality improvement initiative to successfully reduce the frequency of hypoglycemia during treatment of hyperglycemic crises at an academic safety-net hospital: Insights and results","authors":"Katherine L. Modzelewski, Ariana Cannavo , Kathryn L. Fantasia, Sira Korpaisarn , Sara M. Alexanian","doi":"10.1016/j.jcte.2021.100269","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) are potentially life-threatening complications of diabetes. Many hospitals have developed protocols to guide the management of these conditions and align with best practices. One of the main complications encountered in the treatment of hyperglycemic crises is hypoglycemia.</p></div><div><h3>Methods</h3><p>At our institution, we undertook a review of our insulin infusion titration protocol, rates of hypoglycemia, and time to clinical resolution for patients with hyperglycemic crises. A multidisciplinary team performed a literature review and analyzed baseline hospital data with the existing protocol. With the input of multiple stakeholders, several changes were made to the titration algorithm over multiple PDSA cycles to refine the protocol. Effectiveness and safety of the protocol, as well as fidelity with the protocol, were assessed after each PDSA cycle.</p></div><div><h3>Results</h3><p>After the initial cycle, chart review showed a reduction in hypoglycemia rates of more than 50% in patients treated with the new protocol without any increase in time to resolution of DKA. A second version of the protocol was implemented to improve usability, and improvement in hypoglycemia was maintained.</p></div><div><h3>Conclusion</h3><p>Despite the fact that the initial protocol had been developed based on best practice recommendations, rates of hypoglycemia were initially high. Critical assessment of pitfalls in management allowed changes to the protocol that significantly and sustainably reduced hypoglycemia.</p></div>","PeriodicalId":46328,"journal":{"name":"Journal of Clinical and Translational Endocrinology","volume":"26 ","pages":"Article 100269"},"PeriodicalIF":4.2000,"publicationDate":"2021-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d8/87/main.PMC8581574.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Translational Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2214623721000211","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) are potentially life-threatening complications of diabetes. Many hospitals have developed protocols to guide the management of these conditions and align with best practices. One of the main complications encountered in the treatment of hyperglycemic crises is hypoglycemia.
Methods
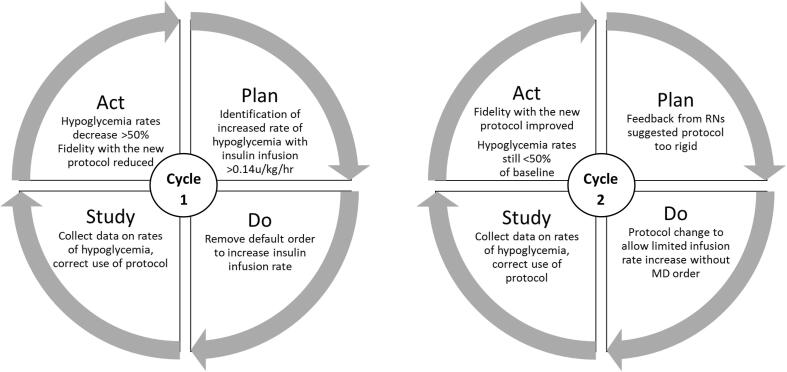
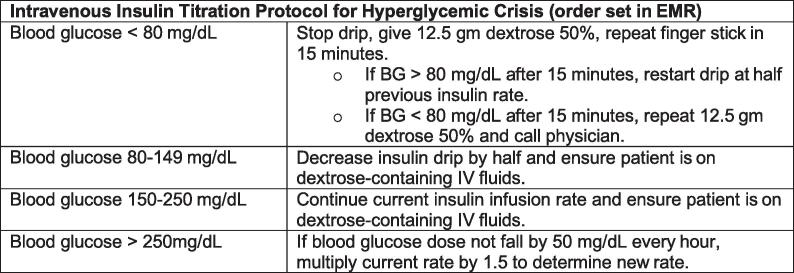
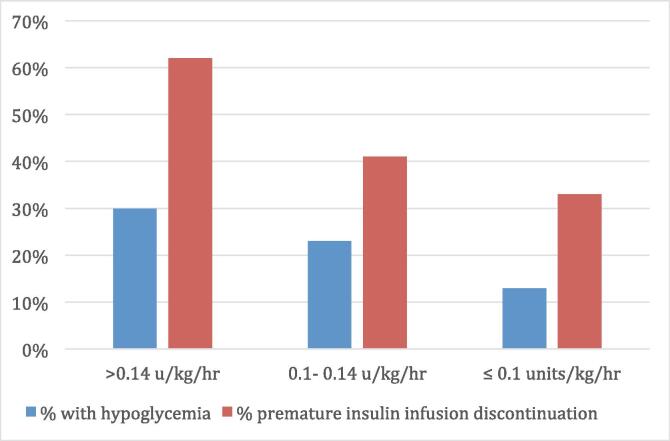
At our institution, we undertook a review of our insulin infusion titration protocol, rates of hypoglycemia, and time to clinical resolution for patients with hyperglycemic crises. A multidisciplinary team performed a literature review and analyzed baseline hospital data with the existing protocol. With the input of multiple stakeholders, several changes were made to the titration algorithm over multiple PDSA cycles to refine the protocol. Effectiveness and safety of the protocol, as well as fidelity with the protocol, were assessed after each PDSA cycle.
Results
After the initial cycle, chart review showed a reduction in hypoglycemia rates of more than 50% in patients treated with the new protocol without any increase in time to resolution of DKA. A second version of the protocol was implemented to improve usability, and improvement in hypoglycemia was maintained.
Conclusion
Despite the fact that the initial protocol had been developed based on best practice recommendations, rates of hypoglycemia were initially high. Critical assessment of pitfalls in management allowed changes to the protocol that significantly and sustainably reduced hypoglycemia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


