{"title":"Kounis Syndrome Secondary to Medicine-Induced Hypersensitivity.","authors":"Parackrama Karunathilake, Udaya Ralapanawa, Thilak Jayalath, Shamali Abeyagunawardena","doi":"10.1155/2021/4485754","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Kounis syndrome is the concurrence of an acute coronary syndrome (ACS) caused by coronary vasospasms, acute myocardial infarctions, or stent thromboses in case of allergic or hypersensitivity reactions. Kounis syndrome is mediated by mast cells that interact with macrophages and T-lymphocytes, causing degranulation and inflammation with cytokine release. It is a life-threatening condition that has many trigger factors and is most commonly caused by medicines. <i>Case Presentation</i>. A 71-year-old male was admitted with a fever of five days' duration associated with cellulitis, for which he had been treated with clindamycin and flucloxacillin before admission. He was a diagnosed patient with hypertension and dyslipidemia five years ago. After taking the antibiotics, he had developed generalized itching followed by urticaria suggesting an allergic reaction. Therefore, he was admitted to the hospital. After admission, he developed an ischaemic-type chest pain associated with autonomic symptoms and shortness of breath. An immediate ECG was taken that showed ST-segment depressions in the chest leads V4-V6, confirmed by a repeat ECG. Troponin I was 8 ng/mL. Acute management of ACS was started, and prednisolone 10 mg daily dose was given. After complete recovery, the patient was discharged with aspirin, clopidogrel, atorvastatin, metoprolol, losartan, isosorbide mononitrate, and nicorandil. Prednisolone 10 mg daily dose was given for five days after discharge.</p><p><strong>Conclusion: </strong>In immediate hypersensitivity, with persistent cardiovascular instability, Kounis syndrome should be considered, and an electrocardiogram and other appropriate assessments and treatments should be initiated. Prompt management of the allergic reaction and the ACS is vital for a better outcome of Kounis syndrome.</p>","PeriodicalId":9627,"journal":{"name":"Case Reports in Medicine","volume":"2021 ","pages":"4485754"},"PeriodicalIF":0.8000,"publicationDate":"2021-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8500773/pdf/","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/4485754","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 5
Abstract
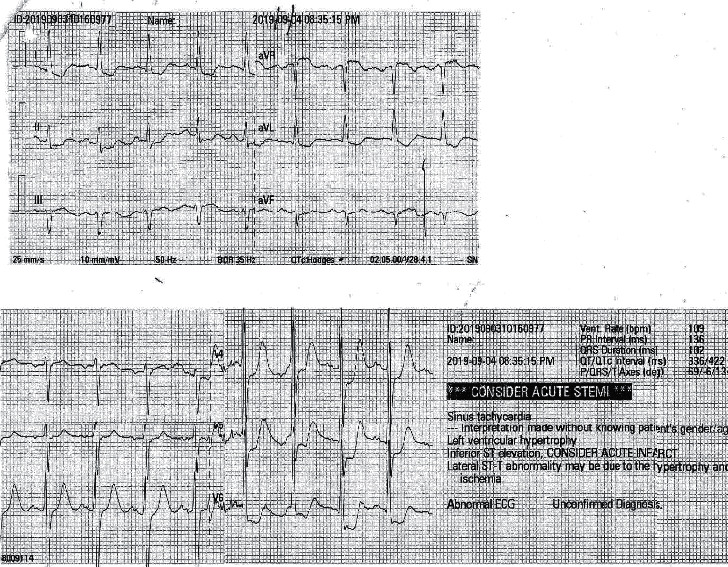
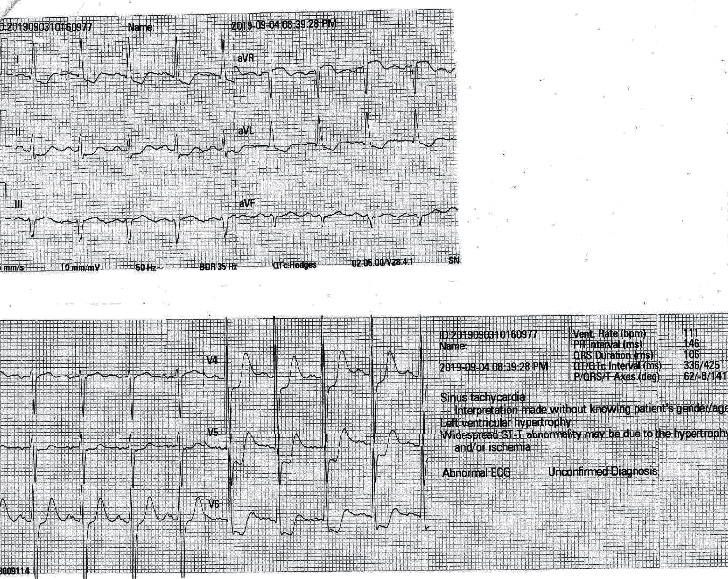
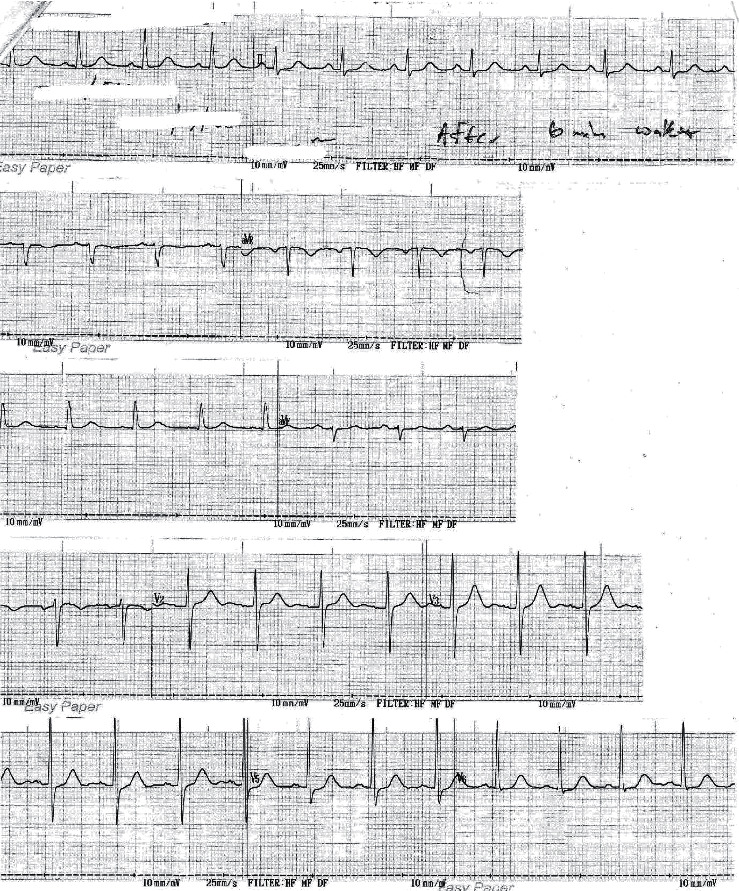
Introduction: Kounis syndrome is the concurrence of an acute coronary syndrome (ACS) caused by coronary vasospasms, acute myocardial infarctions, or stent thromboses in case of allergic or hypersensitivity reactions. Kounis syndrome is mediated by mast cells that interact with macrophages and T-lymphocytes, causing degranulation and inflammation with cytokine release. It is a life-threatening condition that has many trigger factors and is most commonly caused by medicines. Case Presentation. A 71-year-old male was admitted with a fever of five days' duration associated with cellulitis, for which he had been treated with clindamycin and flucloxacillin before admission. He was a diagnosed patient with hypertension and dyslipidemia five years ago. After taking the antibiotics, he had developed generalized itching followed by urticaria suggesting an allergic reaction. Therefore, he was admitted to the hospital. After admission, he developed an ischaemic-type chest pain associated with autonomic symptoms and shortness of breath. An immediate ECG was taken that showed ST-segment depressions in the chest leads V4-V6, confirmed by a repeat ECG. Troponin I was 8 ng/mL. Acute management of ACS was started, and prednisolone 10 mg daily dose was given. After complete recovery, the patient was discharged with aspirin, clopidogrel, atorvastatin, metoprolol, losartan, isosorbide mononitrate, and nicorandil. Prednisolone 10 mg daily dose was given for five days after discharge.
Conclusion: In immediate hypersensitivity, with persistent cardiovascular instability, Kounis syndrome should be considered, and an electrocardiogram and other appropriate assessments and treatments should be initiated. Prompt management of the allergic reaction and the ACS is vital for a better outcome of Kounis syndrome.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


