Nikhil V Kotha, Rohith S Voora, Alex S Qian, Abhishek Kumar, Edmund M Qiao, Tyler F Stewart, Brent S Rose, Ryan K Orosco
{"title":"Prognostic Utility of Pretreatment Neutrophil-Lymphocyte Ratio in Advanced Larynx Cancer.","authors":"Nikhil V Kotha, Rohith S Voora, Alex S Qian, Abhishek Kumar, Edmund M Qiao, Tyler F Stewart, Brent S Rose, Ryan K Orosco","doi":"10.1177/11772719211049848","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Neutrophil-lymphocyte ratio has been explored as a prognosticator in several cancer types, but its association with larynx cancer outcomes is not well known. We aimed to identify an optimal NLR cutoff point and examine the prognostic utility of this biomarker in patients with locoregionally advanced larynx cancer treated with curative intent.</p><p><strong>Methods: </strong>In the Veterans Affairs' (VA) national database, we identified patients with locoregionally advanced (T3-4N0-3M0) laryngeal squamous cell carcinoma diagnosed between 2000 and 2017 and treated with curative intent. NLR cutoff points were calculated using Contal/O'Quigley's method. Outcomes of larynx cancer-specific survival (CSS), overall survival (OS), and non-larynx cancer survival (NCS) were evaluated in multivariable Cox and Fine-Gray models.</p><p><strong>Results: </strong>In 1047 patients, the optimal pretreatment NLR cutoff was identified as 4.17 - 722 patients with NLR ⩽ 4.17, 325 patients with NLR > 4.17. The elevated NLR cohort had a higher proportion of T4 disease (39.4% vs 28.4%), node positive disease (52.3% vs 43.1%), and surgical treatment (43.7% vs 35.2%). In multivariable analysis, NLR > 4.17 was independently associated with worse OS (HR 1.31, 95% CI 1.12-1.54, <i>P</i> = .001) and worse CSS (HR 1.46, 95% CI 1.17-1.83, <i>P</i> < .001), but not with NCS (HR 0.94, 95% CI 0.75-1.18, <i>P</i> = .58).</p><p><strong>Conclusion: </strong>In locoregionally advanced larynx cancer treated with curative intent, we identified elevated NLR to be associated with inferior OS and CSS. Further prospective studies are needed to investigate pretreatment NLR and our identified 4.17 cutoff as a potential larynx cancer-specific marker for this high risk population.</p>","PeriodicalId":47060,"journal":{"name":"Biomarker Insights","volume":"16 ","pages":"11772719211049848"},"PeriodicalIF":2.6000,"publicationDate":"2021-10-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/90/02/10.1177_11772719211049848.PMC8512256.pdf","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomarker Insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11772719211049848","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 4
Abstract
Purpose: Neutrophil-lymphocyte ratio has been explored as a prognosticator in several cancer types, but its association with larynx cancer outcomes is not well known. We aimed to identify an optimal NLR cutoff point and examine the prognostic utility of this biomarker in patients with locoregionally advanced larynx cancer treated with curative intent.
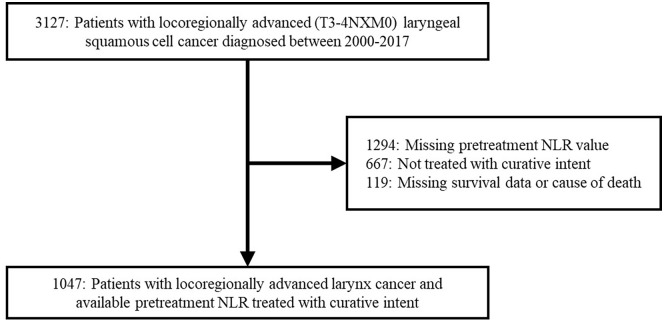
Methods: In the Veterans Affairs' (VA) national database, we identified patients with locoregionally advanced (T3-4N0-3M0) laryngeal squamous cell carcinoma diagnosed between 2000 and 2017 and treated with curative intent. NLR cutoff points were calculated using Contal/O'Quigley's method. Outcomes of larynx cancer-specific survival (CSS), overall survival (OS), and non-larynx cancer survival (NCS) were evaluated in multivariable Cox and Fine-Gray models.
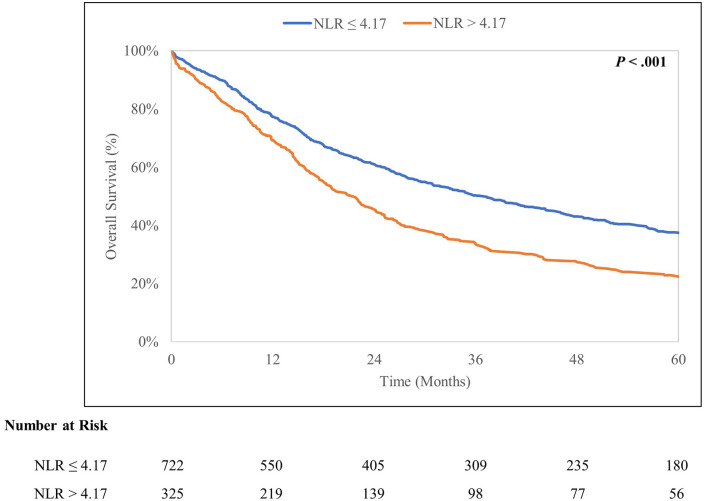
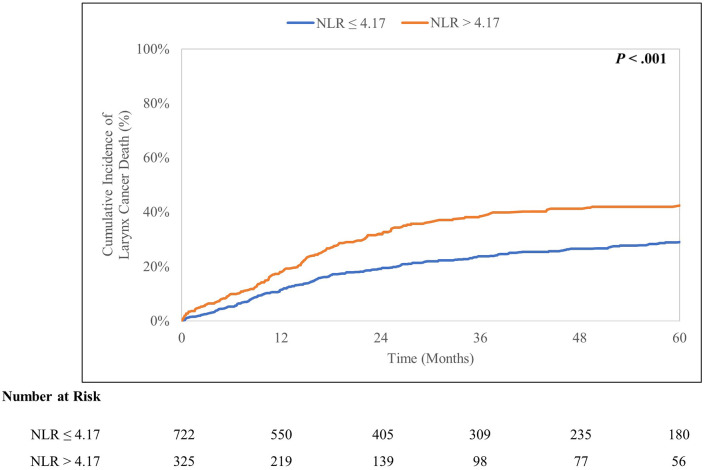
Results: In 1047 patients, the optimal pretreatment NLR cutoff was identified as 4.17 - 722 patients with NLR ⩽ 4.17, 325 patients with NLR > 4.17. The elevated NLR cohort had a higher proportion of T4 disease (39.4% vs 28.4%), node positive disease (52.3% vs 43.1%), and surgical treatment (43.7% vs 35.2%). In multivariable analysis, NLR > 4.17 was independently associated with worse OS (HR 1.31, 95% CI 1.12-1.54, P = .001) and worse CSS (HR 1.46, 95% CI 1.17-1.83, P < .001), but not with NCS (HR 0.94, 95% CI 0.75-1.18, P = .58).
Conclusion: In locoregionally advanced larynx cancer treated with curative intent, we identified elevated NLR to be associated with inferior OS and CSS. Further prospective studies are needed to investigate pretreatment NLR and our identified 4.17 cutoff as a potential larynx cancer-specific marker for this high risk population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


