{"title":"Development of Acute Inflammatory Demyelinating Polyneuropathy 11 Days after Spinal Surgery: A Case Report and Literature Review.","authors":"Eiichi Kakehi, Tadataka Kawakami, Yukiko Ishikawa, Takashi Matsuoka, Naoki Nakagawa, Tugutake Morishita, Shohei Taniguchi, Yukinobu Akamatsu, Shigehisa Sakurai, Akane Hirotani, Takafumi Nozaki, Keisuke Shoji, Seiji Adachi, Kazuhiko Kotani, Masami Matsumura","doi":"10.1155/2021/6283076","DOIUrl":null,"url":null,"abstract":"<p><p>Guillain-Barré syndrome (GBS) usually has a good prognosis; however, patients may develop sequelae without prompt treatment. We herein describe an 81-year-old woman who developed acute-onset excruciating thigh pain and weakness in her lower extremities after spinal surgery. We diagnosed acute inflammatory demyelinating polyradiculoneuropathy by a nerve conduction study, which showed findings of demyelination without cerebrospinal fluid analysis because of a spinal prosthesis. Although anti-GM1 and anti-GalNAc-GD1a antibodies were positive, the patient was clinically diagnosed with acute inflammatory demyelinating polyradiculoneuropathy (a subtype of GBS), not acute motor axonal neuropathy. She recovered well with immunoglobulin therapy. A literature review of 18 cases revealed that unexplained weakness, areflexia, and numbness of the extremities after spinal surgery, a shorter time from spinal surgery to symptom onset to general GBS, abnormal nerve conduction study results, normal spinal imaging findings, and the development of atypical symptoms such as cranial and autonomic nerve syndrome and respiratory failure are useful for diagnosing GBS when cerebrospinal fluid examination cannot be performed after spinal surgery.</p>","PeriodicalId":9627,"journal":{"name":"Case Reports in Medicine","volume":"2021 ","pages":"6283076"},"PeriodicalIF":0.8000,"publicationDate":"2021-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8337157/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/6283076","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
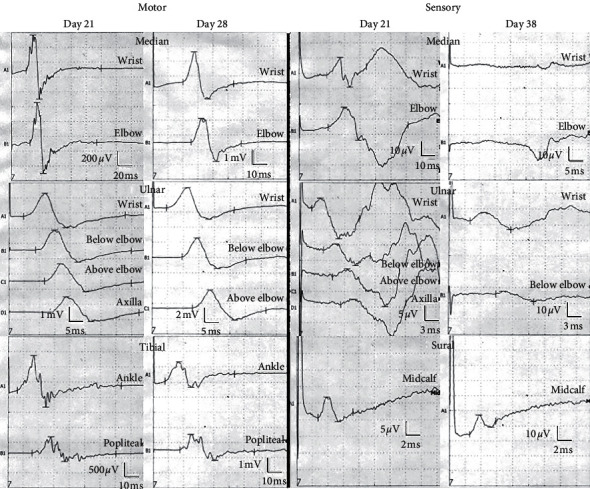
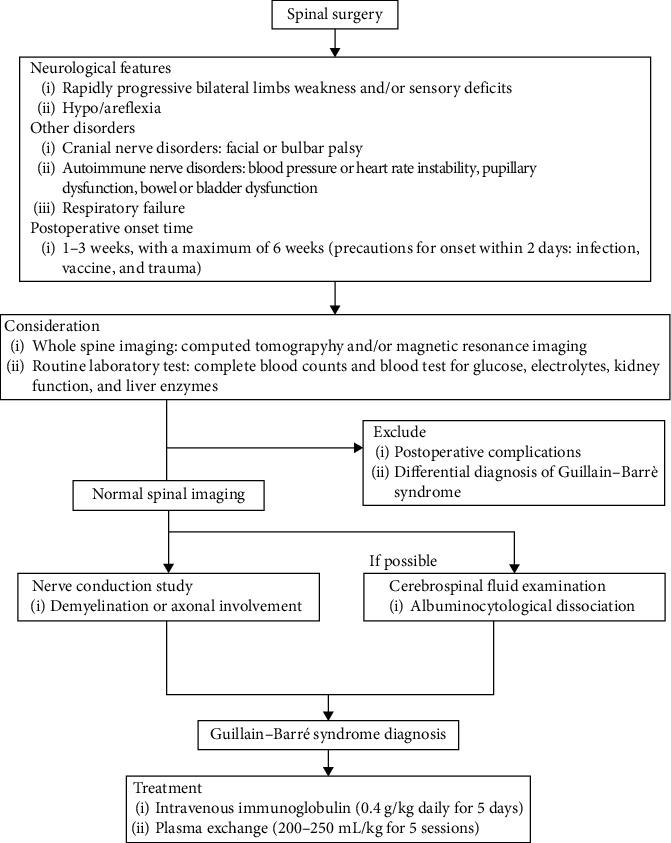
Guillain-Barré syndrome (GBS) usually has a good prognosis; however, patients may develop sequelae without prompt treatment. We herein describe an 81-year-old woman who developed acute-onset excruciating thigh pain and weakness in her lower extremities after spinal surgery. We diagnosed acute inflammatory demyelinating polyradiculoneuropathy by a nerve conduction study, which showed findings of demyelination without cerebrospinal fluid analysis because of a spinal prosthesis. Although anti-GM1 and anti-GalNAc-GD1a antibodies were positive, the patient was clinically diagnosed with acute inflammatory demyelinating polyradiculoneuropathy (a subtype of GBS), not acute motor axonal neuropathy. She recovered well with immunoglobulin therapy. A literature review of 18 cases revealed that unexplained weakness, areflexia, and numbness of the extremities after spinal surgery, a shorter time from spinal surgery to symptom onset to general GBS, abnormal nerve conduction study results, normal spinal imaging findings, and the development of atypical symptoms such as cranial and autonomic nerve syndrome and respiratory failure are useful for diagnosing GBS when cerebrospinal fluid examination cannot be performed after spinal surgery.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


