Effectiveness of Steroid Pulse Therapy for Systemic Side Effects after Bacillus Calmette-Guérin Intravesical Instillation Therapy: A Series of Five Cases.
{"title":"Effectiveness of Steroid Pulse Therapy for Systemic Side Effects after Bacillus Calmette-Guérin Intravesical Instillation Therapy: A Series of Five Cases.","authors":"Tatsuya Umemoto, Jun Naruse, Yukio Usui, Hidenori Zakoji, Hideshi Miyakita, Akira Miyajima","doi":"10.1155/2021/5548054","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Bacillus Calmette-Guérin (BCG) instillation is an established therapy for the treatment of carcinoma in situ (CIS) of the bladder and prevention of recurrence after transurethral resection of bladder tumor noninvasive bladder cancer. However, serious systemic side effects may occur in less than 5% of patients with BCG intravesical instillation. Systemic side effects can sometimes be fatal and require early and accurate treatment. We describe five cases wherein steroid pulse therapy was effective for treating the systemic side effects after BCG intravesical instillation. <i>Case Presentations</i>. BCG intravesical instillation was used to prevent the recurrence of nonmuscle invasive bladder cancer and treat CIS of the bladder; the dose used was 40-80 mg each time, and the Tokyo strain was used. The patients developed fever, impaired consciousness, arthralgia, conjunctival hyperemia, and symptoms of cystitis. The median time from installation to side effect manifestation was 6 days (0-8). One to two courses of steroid pulse therapy were administered (1 course in 3 days), and the dose of methylprednisolone was 500-1000 mg/day. BCG sepsis was observed in one case; however, in the other four cases, one course of steroid pulse therapy showed a rapid improvement in symptoms. In the case of BCG sepsis, hemodialysis and mechanical ventilation were required because of septic shock and acute renal failure. Antituberculosis drugs (isoniazid, rifampicin, and ethambutol) were started promptly; however, no improvement was noticed. Two courses of steroid pulse therapy improved the patient's general condition, and hemodialysis and mechanical ventilation were no longer required. All patients survived without relapse of symptoms.</p><p><strong>Conclusion: </strong>Our cases suggest that early steroid pulse therapy may be effective for rapid symptom improvement of the systemic side effects of BCG instillation therapy.</p>","PeriodicalId":30323,"journal":{"name":"Case Reports in Urology","volume":"2021 ","pages":"5548054"},"PeriodicalIF":0.0000,"publicationDate":"2021-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8286186/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/5548054","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
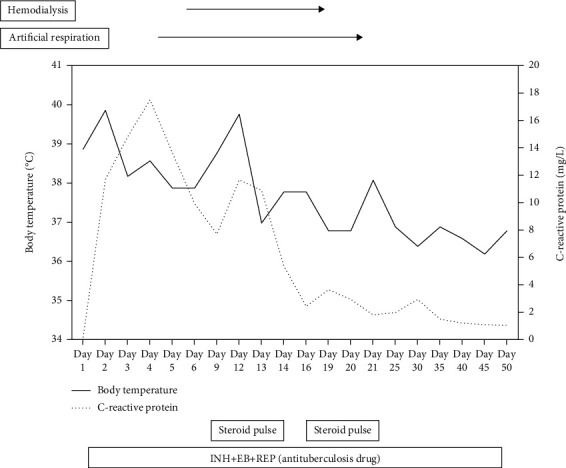
Introduction: Bacillus Calmette-Guérin (BCG) instillation is an established therapy for the treatment of carcinoma in situ (CIS) of the bladder and prevention of recurrence after transurethral resection of bladder tumor noninvasive bladder cancer. However, serious systemic side effects may occur in less than 5% of patients with BCG intravesical instillation. Systemic side effects can sometimes be fatal and require early and accurate treatment. We describe five cases wherein steroid pulse therapy was effective for treating the systemic side effects after BCG intravesical instillation. Case Presentations. BCG intravesical instillation was used to prevent the recurrence of nonmuscle invasive bladder cancer and treat CIS of the bladder; the dose used was 40-80 mg each time, and the Tokyo strain was used. The patients developed fever, impaired consciousness, arthralgia, conjunctival hyperemia, and symptoms of cystitis. The median time from installation to side effect manifestation was 6 days (0-8). One to two courses of steroid pulse therapy were administered (1 course in 3 days), and the dose of methylprednisolone was 500-1000 mg/day. BCG sepsis was observed in one case; however, in the other four cases, one course of steroid pulse therapy showed a rapid improvement in symptoms. In the case of BCG sepsis, hemodialysis and mechanical ventilation were required because of septic shock and acute renal failure. Antituberculosis drugs (isoniazid, rifampicin, and ethambutol) were started promptly; however, no improvement was noticed. Two courses of steroid pulse therapy improved the patient's general condition, and hemodialysis and mechanical ventilation were no longer required. All patients survived without relapse of symptoms.
Conclusion: Our cases suggest that early steroid pulse therapy may be effective for rapid symptom improvement of the systemic side effects of BCG instillation therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


