Ravindra M Vora, Meryl J Alappattu, Apoorva D Zarkar, Mayur S Soni, Santosh J Karmarkar, Aśok C Antony
{"title":"Potential for elimination of folate and vitamin B<sub>12</sub> deficiency in India using vitamin-fortified tea: a preliminary study.","authors":"Ravindra M Vora, Meryl J Alappattu, Apoorva D Zarkar, Mayur S Soni, Santosh J Karmarkar, Aśok C Antony","doi":"10.1136/bmjnph-2020-000209","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The majority of Indian women have a poor dietary folate and vitamin B<sub>12</sub> intake resulting in their chronically low vitamin status, which contributes to anaemia and the high incidence of folate-responsive neural-tube defects (NTDs) in India. Although many countries have successfully deployed centrally-processed folate-fortified flour for prevention of NTDs, inherent logistical problems preclude widespread implementation of this strategy in India. Because tea-the second most common beverage worldwide (after water)-is consumed by most Indians every day, and appeared an ideal vehicle for fortification with folate and vitamin B<sub>12</sub>, we determined if daily consumption of vitamin-fortified tea for 2 months could benefit young women of childbearing-age in Sangli, India.</p><p><strong>Methods: </strong>Women (average age=20±2 SD) used teabags spiked with therapeutic doses of 1 mg folate plus <i>either</i> 0.1 mg vitamin B<sub>12</sub> (Group-1, n=<i>19</i>) <i>or</i> 0.5 mg vitamin B<sub>12</sub> (Group-2, n=<i>19</i>), or mock-fortified teabags (Group-0, n=<i>5</i>) to prepare a cup of tea every day for 2 months, following which their pre-intervention and post-intervention serum vitamin and haemoglobin concentrations were compared.</p><p><strong>Results: </strong>Most women had baseline anaemia with low-normal serum folate and below-normal serum vitamin B<sub>12</sub> levels. After 2 months, women in both Group-1 and Group-2 exhibited significant increases in mean differences in pre-intervention versus post-intervention serum folate levels of 8.37 ng/mL (95% CIs 5.69 to 11.04, p<0.05) and 6.69 ng/mL (95% CI 3.93 to 9.44, p<0.05), respectively; however, Group-0 experienced an insignificant rise of 1.26 ng/mL (95% CI -4.08 to 0.16). In addition, over one-half and two-thirds of women in Group-1 and Group-2, respectively, exhibited increases in serum vitamin B<sub>12</sub> levels over 300 pg/mL. There was also a significant post-interventional increase in the mean haemoglobin concentration in Group-1 of 1.45 g/dL (95% CI 0.64 to 2.26, p=0.002) and Group-2 of 0.79 g/dL (95% CI 0.11 to 1.42, p=0.027), which reflected a bona fide clinical response.</p><p><strong>Conclusion: </strong>Tea is an outstanding scalable vehicle for fortification with folate and vitamin B<sub>12</sub> in India, and has potential to help eliminate haematological and neurological complications arising from inadequate dietary consumption or absorption of folate and vitamin B<sub>12</sub>.</p>","PeriodicalId":36307,"journal":{"name":"BMJ Nutrition, Prevention and Health","volume":" ","pages":"293-306"},"PeriodicalIF":2.5000,"publicationDate":"2021-06-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1136/bmjnph-2020-000209","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Nutrition, Prevention and Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjnph-2020-000209","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"NUTRITION & DIETETICS","Score":null,"Total":0}
引用次数: 8
Abstract
Introduction: The majority of Indian women have a poor dietary folate and vitamin B12 intake resulting in their chronically low vitamin status, which contributes to anaemia and the high incidence of folate-responsive neural-tube defects (NTDs) in India. Although many countries have successfully deployed centrally-processed folate-fortified flour for prevention of NTDs, inherent logistical problems preclude widespread implementation of this strategy in India. Because tea-the second most common beverage worldwide (after water)-is consumed by most Indians every day, and appeared an ideal vehicle for fortification with folate and vitamin B12, we determined if daily consumption of vitamin-fortified tea for 2 months could benefit young women of childbearing-age in Sangli, India.
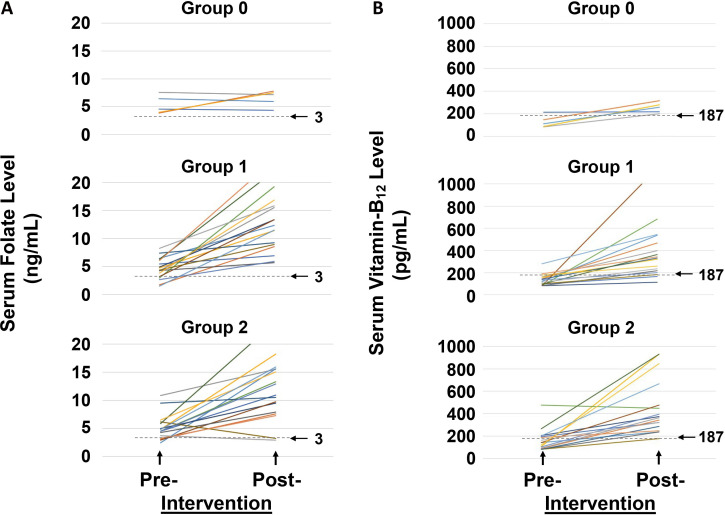
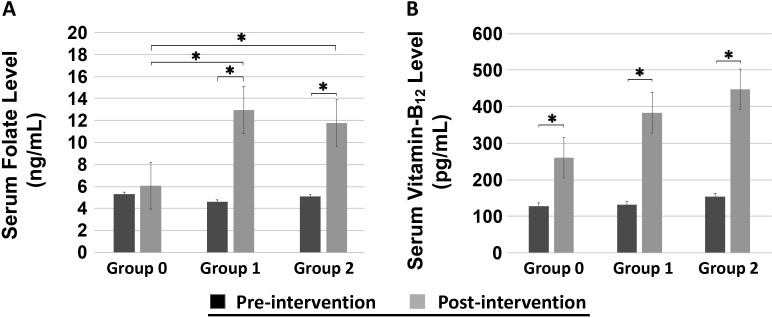
Methods: Women (average age=20±2 SD) used teabags spiked with therapeutic doses of 1 mg folate plus either 0.1 mg vitamin B12 (Group-1, n=19) or 0.5 mg vitamin B12 (Group-2, n=19), or mock-fortified teabags (Group-0, n=5) to prepare a cup of tea every day for 2 months, following which their pre-intervention and post-intervention serum vitamin and haemoglobin concentrations were compared.
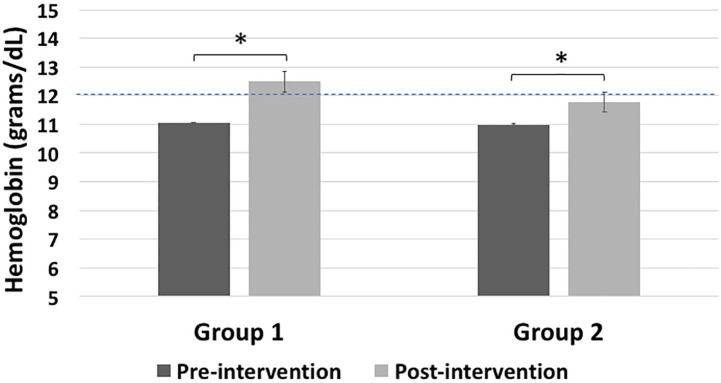
Results: Most women had baseline anaemia with low-normal serum folate and below-normal serum vitamin B12 levels. After 2 months, women in both Group-1 and Group-2 exhibited significant increases in mean differences in pre-intervention versus post-intervention serum folate levels of 8.37 ng/mL (95% CIs 5.69 to 11.04, p<0.05) and 6.69 ng/mL (95% CI 3.93 to 9.44, p<0.05), respectively; however, Group-0 experienced an insignificant rise of 1.26 ng/mL (95% CI -4.08 to 0.16). In addition, over one-half and two-thirds of women in Group-1 and Group-2, respectively, exhibited increases in serum vitamin B12 levels over 300 pg/mL. There was also a significant post-interventional increase in the mean haemoglobin concentration in Group-1 of 1.45 g/dL (95% CI 0.64 to 2.26, p=0.002) and Group-2 of 0.79 g/dL (95% CI 0.11 to 1.42, p=0.027), which reflected a bona fide clinical response.
Conclusion: Tea is an outstanding scalable vehicle for fortification with folate and vitamin B12 in India, and has potential to help eliminate haematological and neurological complications arising from inadequate dietary consumption or absorption of folate and vitamin B12.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


