F Flottmann, N van Horn, M E Maros, R McDonough, M Deb-Chatterji, A Alegiani, G Thomalla, U Hanning, J Fiehler, C Brekenfeld
{"title":"Early TICI 2b or Late TICI 3-Is Perfect the Enemy of Good?","authors":"F Flottmann, N van Horn, M E Maros, R McDonough, M Deb-Chatterji, A Alegiani, G Thomalla, U Hanning, J Fiehler, C Brekenfeld","doi":"10.1007/s00062-021-01048-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>A Thrombolysis in Cerebral Infarction (TICI) score of 3 has been established as therapeutic goal in endovascular therapy (EVT) for acute ischemic stroke; however, in the case of early TICI2b reperfusion, the question remains whether to stop the procedure or to continue in the pursuit of perfection (i.e., TICI 2c/3).</p><p><strong>Methods: </strong>A total of 6635 patients were screened from the German Stroke Registry. Patients who underwent EVT for occlusion of the middle cerebral artery (M1 segment), with final TICI score of 2b/3 were included. Multivariable logistic regression was performed with functional independence (modified Rankin Scale, mRS at day 90 of 0-2) as the dependent variable.</p><p><strong>Results: </strong>Of 1497 patients, 586 (39.1%) met inclusion criteria with a final TICI score of 2b and 911 (60.9%) with a TICI score of 3. Patients who achieved first-pass TICI3 showed highest odds of functional independence (Odds ratio [OR] 1.71, 95% confidence interval [95% CI] 1.18-2.47). Patients who achieved TICI2b with the second pass (OR 0.53, 95% CI 0.31-0.89) or with three or more passes (OR 0.44, 95% CI 0.27-0.70) had significantly worse clinical outcomes compared to first-pass TICI2b. TICI3 at the second pass was by trend better than first-pass TICI2b (OR 1.55, 95% CI 0.98-2.45), but TICI3 after 3 or more passes (OR 0.93, 95% CI 0.57-1.50) was not significantly different from first-pass TICI2b.</p><p><strong>Conclusion: </strong>First-pass TICI2b was superior to TICI2b after ≥ 2 retrievals and comparable to TICI3 at ≥ 3 retrievals. The potential benefit in outcome after achieving TICI3 following further retrieval attempts after first-pass TICI2b need to be weighed against the risks.</p>","PeriodicalId":49298,"journal":{"name":"Clinical Neuroradiology","volume":"32 2","pages":"353-360"},"PeriodicalIF":2.4000,"publicationDate":"2022-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s00062-021-01048-8","citationCount":"11","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Neuroradiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00062-021-01048-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/6/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 11
Abstract
Background and purpose: A Thrombolysis in Cerebral Infarction (TICI) score of 3 has been established as therapeutic goal in endovascular therapy (EVT) for acute ischemic stroke; however, in the case of early TICI2b reperfusion, the question remains whether to stop the procedure or to continue in the pursuit of perfection (i.e., TICI 2c/3).
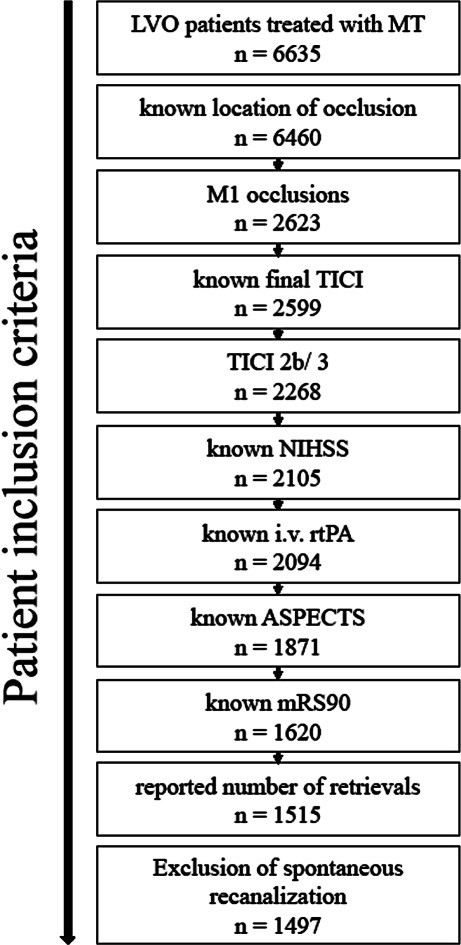
Methods: A total of 6635 patients were screened from the German Stroke Registry. Patients who underwent EVT for occlusion of the middle cerebral artery (M1 segment), with final TICI score of 2b/3 were included. Multivariable logistic regression was performed with functional independence (modified Rankin Scale, mRS at day 90 of 0-2) as the dependent variable.
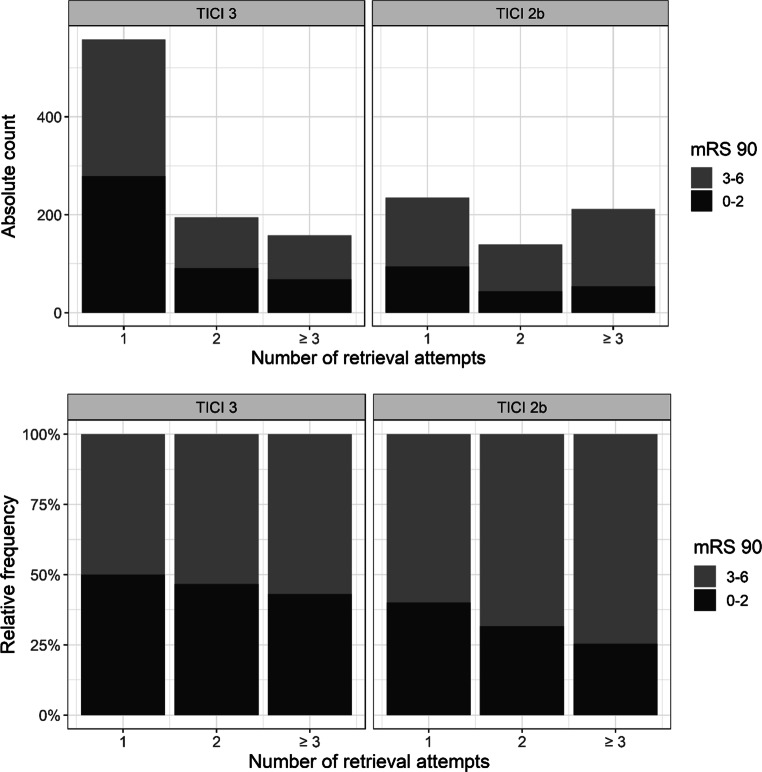
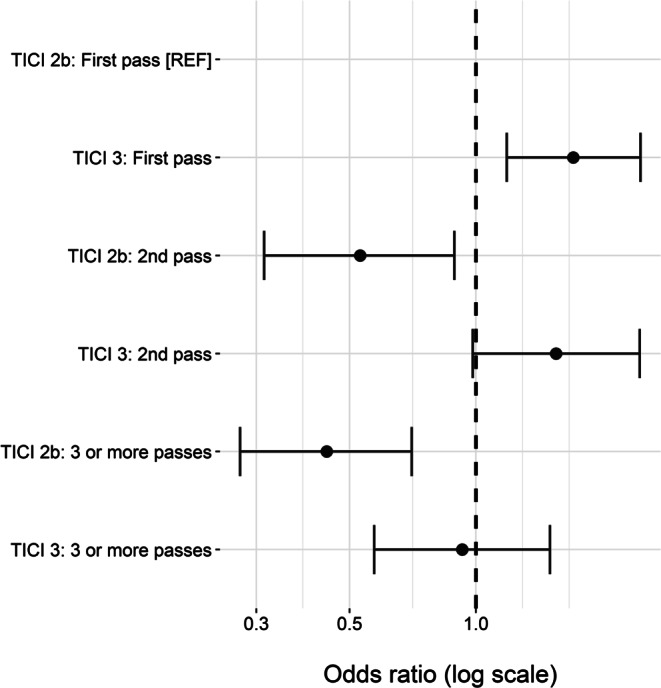
Results: Of 1497 patients, 586 (39.1%) met inclusion criteria with a final TICI score of 2b and 911 (60.9%) with a TICI score of 3. Patients who achieved first-pass TICI3 showed highest odds of functional independence (Odds ratio [OR] 1.71, 95% confidence interval [95% CI] 1.18-2.47). Patients who achieved TICI2b with the second pass (OR 0.53, 95% CI 0.31-0.89) or with three or more passes (OR 0.44, 95% CI 0.27-0.70) had significantly worse clinical outcomes compared to first-pass TICI2b. TICI3 at the second pass was by trend better than first-pass TICI2b (OR 1.55, 95% CI 0.98-2.45), but TICI3 after 3 or more passes (OR 0.93, 95% CI 0.57-1.50) was not significantly different from first-pass TICI2b.
Conclusion: First-pass TICI2b was superior to TICI2b after ≥ 2 retrievals and comparable to TICI3 at ≥ 3 retrievals. The potential benefit in outcome after achieving TICI3 following further retrieval attempts after first-pass TICI2b need to be weighed against the risks.
期刊介绍:
Clinical Neuroradiology provides current information, original contributions, and reviews in the field of neuroradiology. An interdisciplinary approach is accomplished by diagnostic and therapeutic contributions related to associated subjects.
The international coverage and relevance of the journal is underlined by its being the official journal of the German, Swiss, and Austrian Societies of Neuroradiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


