High HIV-1 Virological Failure and Drug Resistance among Adult Patients Receiving First-Line ART for At least 12 Months at a Decentralized Urban HIV Clinic Setting in Senegal before the Test-and-Treat.
{"title":"High HIV-1 Virological Failure and Drug Resistance among Adult Patients Receiving First-Line ART for At least 12 Months at a Decentralized Urban HIV Clinic Setting in Senegal before the Test-and-Treat.","authors":"Aristid Ekollo Mbange, Abou Abdallah Malick Diouara, Halimatou Diop-Ndiaye, Ndèye Aminata Diaw Diouf, Ndèye Fatou Ngom-Ngueye, Kine Ndiaye Touré, Ahmed Dieng, Seynabou Lô, Mamadou Fall, Wilfred Fon Mbacham, Souleymane Mboup, Coumba Touré-Kane","doi":"10.1177/11786337211014503","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The feasibility of antiretroviral therapy (ART) monitoring remains problematic in decentralized HIV clinic settings of sub-Saharan Africa. We assessed the rates and correlates of HIV-1 virological failure (VF) and drug resistance (DR) in 2 pre-test-and-treat urban clinic settings of Senegal.</p><p><strong>Methods: </strong>Consenting HIV-1-infected adults (⩾18 years) receiving first-line ART for ⩾12 months were cross-sectionally enrolled between January and March 2015, at the referral outpatient treatment center of Dakar (n = 151) and decentralized regional hospital of Saint-Louis (n = 127). In the 12 months preceding plasma specimens' collection patients at Saint-Louis had no viral load (VL) testing. Significant predictors of VF (VL ⩾ 1000 copies/ml) and DR (clinically relevant mutations) were determined using binomial logistic regression in R software.</p><p><strong>Results: </strong>Of the 278 adults on EFV-/NVP-based regimens, 32 (11.5% [95%CI: 8.0-15.9]) experienced VF. Failing and non-failing patients had comparable median time [interquartile] on ART (69.5 [23.0-89.5] vs 64.0 [34.0-99.0] months; <i>P</i> = .46, Mann-Whitney <i>U</i>-test). Of the 27 viraemic isolates successfully genotyped, 20 (74.1%) carried DR mutations; most frequent were M184VI (55.6%), K103N (37.1%), thymidine analog mutations (29.6%), Y181CY (22.2%). The pattern of mutations did not always correspond to the ongoing treatment. The adjusted odds of VF was significantly associated with the decentralized clinic site (<i>P</i> < .001) and CD4 < 350 cells/mm<sup>3</sup> (<i>P</i> < .006). Strong correlates of DR also included Saint-Louis (<i>P</i> < .009), CD4 < 350 cells/mm<sup>3</sup> (<i>P</i> <. 001), and nevirapine-based therapies (comparator: efavirenz-based therapies; <i>P</i> < .027). In stratification analyses by site, higher rate of VF at Saint-Louis (20.5% [95%CI: 13.8-28.5] vs 4.0% [95%CI: 1.5-8.5] in Dakar) was associated with nevirapine-based therapies (OR = 3.34 [1.07-11.75], <i>P</i> = .038), self-reported missing doses (OR = 3.30 [1.13-10.24], <i>P</i> = .029), and medical appointments (OR = 2.91 [1.05-8.47], <i>P</i> = .039) in the last 1 and 12 months(s), respectively. The higher rate of DR at Saint-Louis (12.9% [95%CI: 7.6-20.1] vs 2.7% [95%CI: 0.7-6.7] in Dakar) was associated with nevirapine-based therapies (OR = 5.13 [1.12-37.35], <i>P</i> = .035).</p><p><strong>Conclusion: </strong>At decentralized urban settings, there is need for enhanced virological monitoring and adherence support. HIV programs in Senegal should intensify early HIV diagnosis for effective test-and-treat. These interventions, in addition to the superiority of efavirenz-based therapies provide a favorable framework for transitioning to the recommended potent drug dolutegravir, thereby ensuring its long-term use.</p>","PeriodicalId":13671,"journal":{"name":"Infectious Diseases","volume":"14 ","pages":"11786337211014503"},"PeriodicalIF":2.3000,"publicationDate":"2021-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/aa/d3/10.1177_11786337211014503.PMC8120520.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/11786337211014503","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The feasibility of antiretroviral therapy (ART) monitoring remains problematic in decentralized HIV clinic settings of sub-Saharan Africa. We assessed the rates and correlates of HIV-1 virological failure (VF) and drug resistance (DR) in 2 pre-test-and-treat urban clinic settings of Senegal.
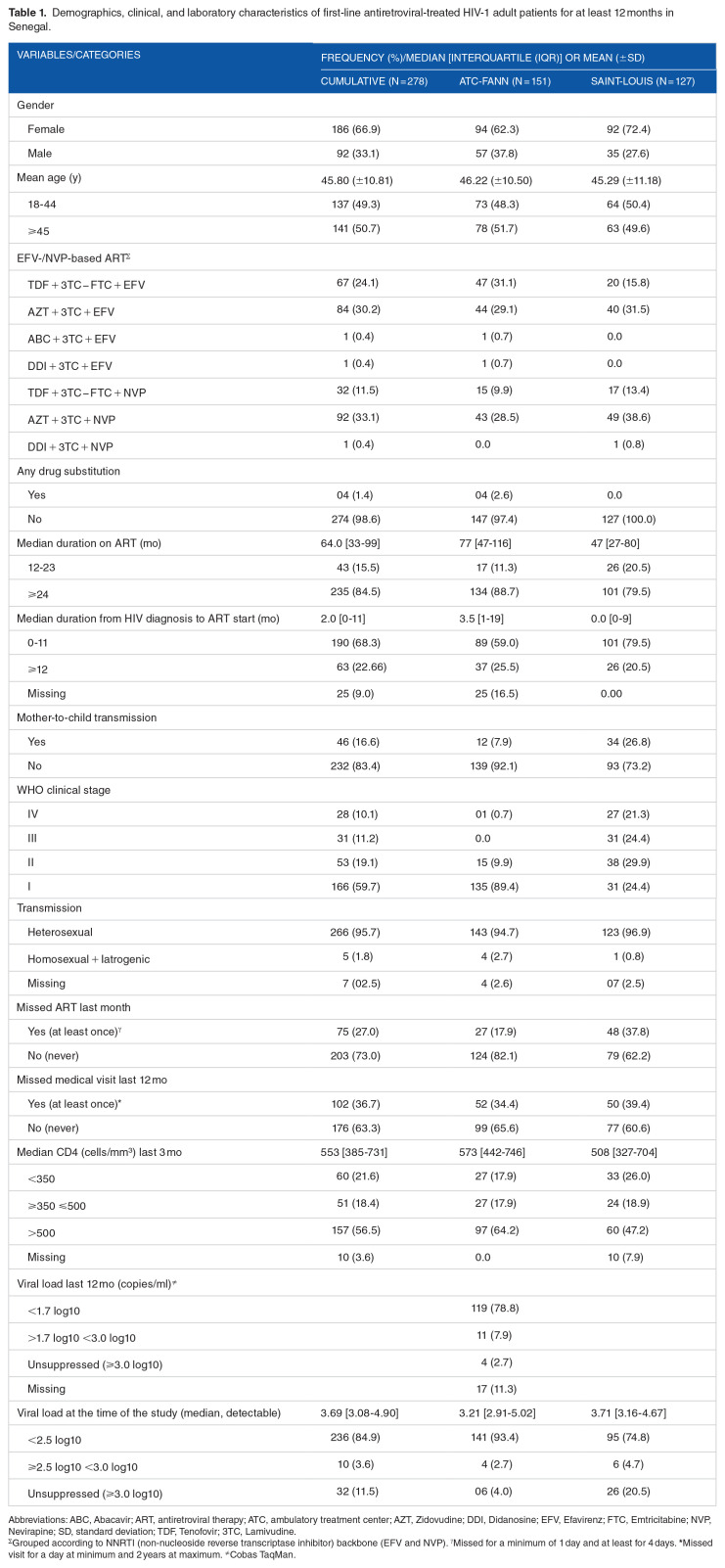
Methods: Consenting HIV-1-infected adults (⩾18 years) receiving first-line ART for ⩾12 months were cross-sectionally enrolled between January and March 2015, at the referral outpatient treatment center of Dakar (n = 151) and decentralized regional hospital of Saint-Louis (n = 127). In the 12 months preceding plasma specimens' collection patients at Saint-Louis had no viral load (VL) testing. Significant predictors of VF (VL ⩾ 1000 copies/ml) and DR (clinically relevant mutations) were determined using binomial logistic regression in R software.
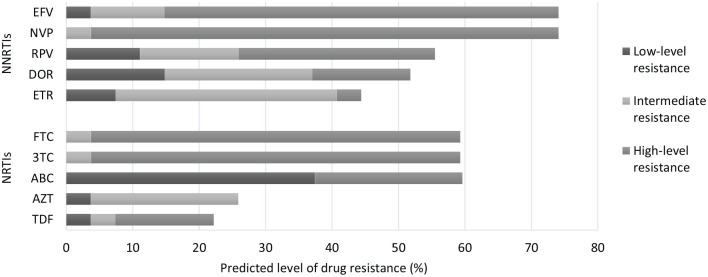
Results: Of the 278 adults on EFV-/NVP-based regimens, 32 (11.5% [95%CI: 8.0-15.9]) experienced VF. Failing and non-failing patients had comparable median time [interquartile] on ART (69.5 [23.0-89.5] vs 64.0 [34.0-99.0] months; P = .46, Mann-Whitney U-test). Of the 27 viraemic isolates successfully genotyped, 20 (74.1%) carried DR mutations; most frequent were M184VI (55.6%), K103N (37.1%), thymidine analog mutations (29.6%), Y181CY (22.2%). The pattern of mutations did not always correspond to the ongoing treatment. The adjusted odds of VF was significantly associated with the decentralized clinic site (P < .001) and CD4 < 350 cells/mm3 (P < .006). Strong correlates of DR also included Saint-Louis (P < .009), CD4 < 350 cells/mm3 (P <. 001), and nevirapine-based therapies (comparator: efavirenz-based therapies; P < .027). In stratification analyses by site, higher rate of VF at Saint-Louis (20.5% [95%CI: 13.8-28.5] vs 4.0% [95%CI: 1.5-8.5] in Dakar) was associated with nevirapine-based therapies (OR = 3.34 [1.07-11.75], P = .038), self-reported missing doses (OR = 3.30 [1.13-10.24], P = .029), and medical appointments (OR = 2.91 [1.05-8.47], P = .039) in the last 1 and 12 months(s), respectively. The higher rate of DR at Saint-Louis (12.9% [95%CI: 7.6-20.1] vs 2.7% [95%CI: 0.7-6.7] in Dakar) was associated with nevirapine-based therapies (OR = 5.13 [1.12-37.35], P = .035).
Conclusion: At decentralized urban settings, there is need for enhanced virological monitoring and adherence support. HIV programs in Senegal should intensify early HIV diagnosis for effective test-and-treat. These interventions, in addition to the superiority of efavirenz-based therapies provide a favorable framework for transitioning to the recommended potent drug dolutegravir, thereby ensuring its long-term use.
期刊介绍:
Infectious Diseases (formerly Scandinavian Journal of Infectious Diseases) is a peer-reviewed journal publishing articles on all aspects of human infection, including pathogenesis, diagnosis, and treatment of infectious diseases, and also on medical microbiology and epidemiology

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


