Mitral early-diastolic inflow peak velocity (E)-to-left atrial strain ratio as a novel index for predicting elevated left ventricular filling pressures in patients with preserved left ventricular ejection fraction.
You Zhou, Cai-Ming Zhao, Zhen-Ya Shen, Xin Zhao, Bing-Yuan Zhou
{"title":"Mitral early-diastolic inflow peak velocity (E)-to-left atrial strain ratio as a novel index for predicting elevated left ventricular filling pressures in patients with preserved left ventricular ejection fraction.","authors":"You Zhou, Cai-Ming Zhao, Zhen-Ya Shen, Xin Zhao, Bing-Yuan Zhou","doi":"10.1186/s12947-021-00248-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>We sought to explore the relationship between an index of left ventricular diastolic function parameters combined with left atrial strain and the diastolic function of patients with preserved ejection fraction.</p><p><strong>Methods: </strong>We prospectively enrolled 388 patients with left ventricular ejection fraction (LVEF) ≥ 50%, 49 of whom underwent left heart catherization. Transthoracic echocardiography was performed within 12 h before or after the procedure. Left atrial (LA) strain was obtained by speckle tracking echocardiography. These patients served as the test group. The remaining patients (n = 339) were used to validate the diagnostic performance of the mitral early-diastolic inflow peak velocity (E)-to-left atrial reservoir strain ratio (E/LASr) in left ventricular diastolic dysfunction.</p><p><strong>Results: </strong>Invasive measurements of LV end-diastolic pressure (LVEDP) demonstrated that the E/LASr ratio was increased in patients with elevated LVEDP [ 2.0 (1.8-2.2) vs 3.0 (2.6-4.0), p < 0.001] in the test group (n = 49). After adjusting for age, mitral A, E/e' ratio and β-blocker use, the E/LASr ratio was an independent predictor of elevated LVEDP and showed good diagnostic performance in determining elevated LVEDP [area under the curve (AUC) 0.903, cutoff value 2.7, sensitivity 74.2%, specificity 94.4%]. In the validation group (n = 339), the E/LASr ratio also performed well in diagnosing elevated left atrial pressure (LAP) (AUC 0.904, cutoff value 3.2, sensitivity 76.5%, specificity 89.0%), while with a cut-off value of 2.7, the E/LASr ratio showed high accuracy in discriminating elevated LAP. In addition, E/LASr was a good index of excellent diagnostic utility (AUC: 0.899 to 0.996) in the categorization of diastolic dysfunction grades. Regarding the clinical relevance of this index, the E/LASr ratio could accurately diagnose HF with preserved ejection fraction (HFpEF) (0.781), especially in patients with \"indeterminate\" status (AUC: 0.829). Furthermore, an elevated E/LASr ratio was significantly associated with the risk of rehospitalization due to major adverse cardiac events (MACEs) within one year (odds ratio: 1.183, 95% confidence interval: 1.067, 1.312).</p><p><strong>Conclusions: </strong>In patients with EF preservation, the E/LASr ratio is a novel index for assessing elevated left ventricular filling pressure with high accuracy.</p>","PeriodicalId":9613,"journal":{"name":"Cardiovascular Ultrasound","volume":"19 1","pages":"17"},"PeriodicalIF":1.9000,"publicationDate":"2021-04-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s12947-021-00248-z","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Ultrasound","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12947-021-00248-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 3
Abstract
Objectives: We sought to explore the relationship between an index of left ventricular diastolic function parameters combined with left atrial strain and the diastolic function of patients with preserved ejection fraction.
Methods: We prospectively enrolled 388 patients with left ventricular ejection fraction (LVEF) ≥ 50%, 49 of whom underwent left heart catherization. Transthoracic echocardiography was performed within 12 h before or after the procedure. Left atrial (LA) strain was obtained by speckle tracking echocardiography. These patients served as the test group. The remaining patients (n = 339) were used to validate the diagnostic performance of the mitral early-diastolic inflow peak velocity (E)-to-left atrial reservoir strain ratio (E/LASr) in left ventricular diastolic dysfunction.
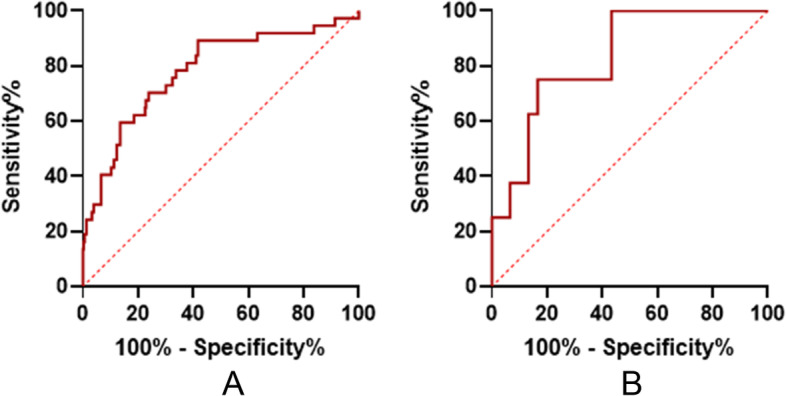
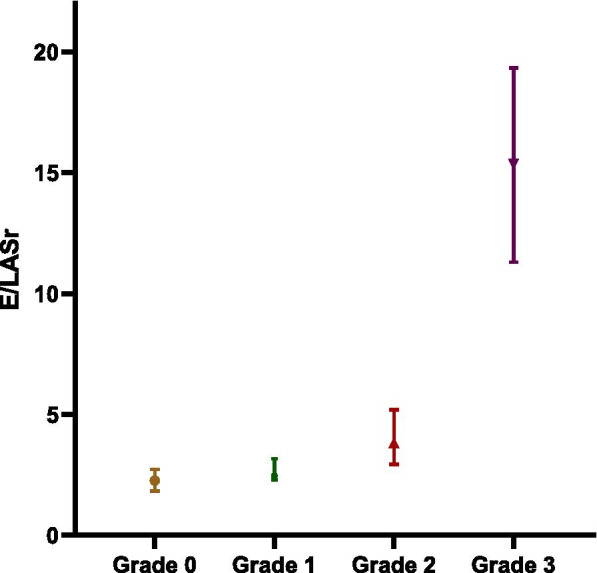
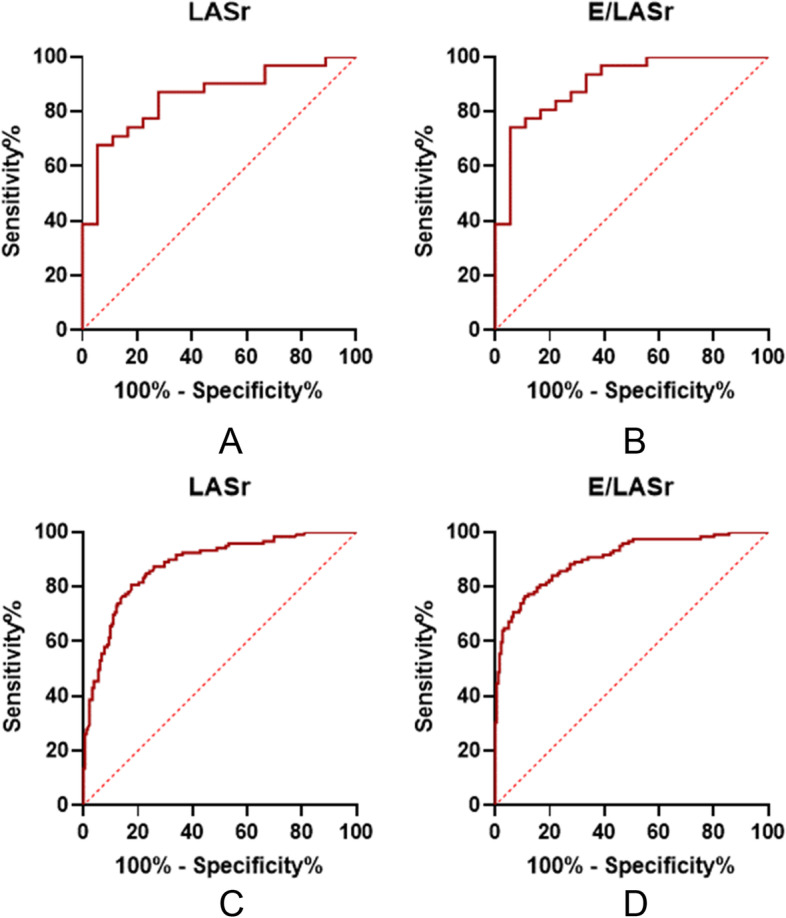
Results: Invasive measurements of LV end-diastolic pressure (LVEDP) demonstrated that the E/LASr ratio was increased in patients with elevated LVEDP [ 2.0 (1.8-2.2) vs 3.0 (2.6-4.0), p < 0.001] in the test group (n = 49). After adjusting for age, mitral A, E/e' ratio and β-blocker use, the E/LASr ratio was an independent predictor of elevated LVEDP and showed good diagnostic performance in determining elevated LVEDP [area under the curve (AUC) 0.903, cutoff value 2.7, sensitivity 74.2%, specificity 94.4%]. In the validation group (n = 339), the E/LASr ratio also performed well in diagnosing elevated left atrial pressure (LAP) (AUC 0.904, cutoff value 3.2, sensitivity 76.5%, specificity 89.0%), while with a cut-off value of 2.7, the E/LASr ratio showed high accuracy in discriminating elevated LAP. In addition, E/LASr was a good index of excellent diagnostic utility (AUC: 0.899 to 0.996) in the categorization of diastolic dysfunction grades. Regarding the clinical relevance of this index, the E/LASr ratio could accurately diagnose HF with preserved ejection fraction (HFpEF) (0.781), especially in patients with "indeterminate" status (AUC: 0.829). Furthermore, an elevated E/LASr ratio was significantly associated with the risk of rehospitalization due to major adverse cardiac events (MACEs) within one year (odds ratio: 1.183, 95% confidence interval: 1.067, 1.312).
Conclusions: In patients with EF preservation, the E/LASr ratio is a novel index for assessing elevated left ventricular filling pressure with high accuracy.
期刊介绍:
Cardiovascular Ultrasound is an online journal, publishing peer-reviewed: original research; authoritative reviews; case reports on challenging and/or unusual diagnostic aspects; and expert opinions on new techniques and technologies. We are particularly interested in articles that include relevant images or video files, which provide an additional dimension to published articles and enhance understanding.
As an open access journal, Cardiovascular Ultrasound ensures high visibility for authors in addition to providing an up-to-date and freely available resource for the community. The journal welcomes discussion, and provides a forum for publishing opinion and debate ranging from biology to engineering to clinical echocardiography, with both speed and versatility.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


