Gary Mikhjian, Ahmad Elghoroury, Keith Cronovich, Kevin Brody, Robert Jarski
{"title":"Using Quantitative D-Dimer to Determine the Need for Pulmonary CT Angiography in COVID-19 Patients.","authors":"Gary Mikhjian, Ahmad Elghoroury, Keith Cronovich, Kevin Brody, Robert Jarski","doi":"10.51894/001c.18652","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>COVID-19 has been frequently cited as a condition causing a pro-inflammatory state leading to hypercoagulopathy and increased risk for venous thromboembolism. This condition has thus prompted prior studies and screening models that utilize D-dimer for pulmonary embolism (PE) into question. The limited research to date has failed to provide tools or guidance regarding what COVID-19 positive patients should receive pulmonary CT angiography screening. This knowledge gap has led to missed diagnoses, CT overutilization, and increased morbidity and mortality.</p><p><strong>Objective: </strong>The purpose of this study was to examine the utility of the quantitative D-dimer lab marker in a convenience sample of 426 COVID-19 positive patients to assist providers in determining the utility of pulmonary CT angiography.</p><p><strong>Methods: </strong>The authors conducted a retrospective analysis on all COVID-19 positive patients within the Henry Ford Medical System between March 1st, 2020 through April 30th, 2020 who received pulmonary CT angiography and had a quantitative D-dimer lab drawn within 24 hours of CT imaging.</p><p><strong>Results: </strong>Our sampling criteria yielded a total of n = 426 patients, of whom 347 (81.5%) were negative for PE and 79 (18.5%) were positive for PE. The average D-dimer in the negative PE group was 2.95 μg./mL. (SD 4.26), significantly different than the 9.15 μg./mL. (SD 6.80) positive PE group (P < 0.05; 95% CI -7.8, -4.6). Theoretically, applying the traditional ≤ 0.5 μg./mL. D-dimer cut-off to our data would yield a sensitivity of 100% and specificity of 7.49% for exclusion of PE. Based on these results, the authors would be able to increase the D-dimer threshold to < 0.89 μg./mL. to maintain their sensitivity to 100% and raise the specificity to 27.95%. Observing a D-dimer cut-off value of ≤ 1.28 μg./mL. would reduce sensitivity to 97.47% but increase the specificity to 57.93%.</p><p><strong>Conclusions: </strong>These study results support the utilization of alternative D-dimer thresholds to exclude PE in COVID-19 patients. Based on these findings, providers may be able to observe increased D-dimer cut-off values to reduce unnecessary pulmonary CT angiography scans.</p>","PeriodicalId":74853,"journal":{"name":"Spartan medical research journal","volume":"6 1","pages":"18652"},"PeriodicalIF":0.0000,"publicationDate":"2021-04-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8043904/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spartan medical research journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.51894/001c.18652","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: COVID-19 has been frequently cited as a condition causing a pro-inflammatory state leading to hypercoagulopathy and increased risk for venous thromboembolism. This condition has thus prompted prior studies and screening models that utilize D-dimer for pulmonary embolism (PE) into question. The limited research to date has failed to provide tools or guidance regarding what COVID-19 positive patients should receive pulmonary CT angiography screening. This knowledge gap has led to missed diagnoses, CT overutilization, and increased morbidity and mortality.
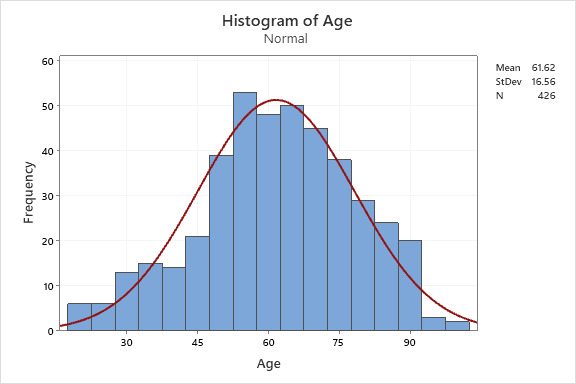
Objective: The purpose of this study was to examine the utility of the quantitative D-dimer lab marker in a convenience sample of 426 COVID-19 positive patients to assist providers in determining the utility of pulmonary CT angiography.
Methods: The authors conducted a retrospective analysis on all COVID-19 positive patients within the Henry Ford Medical System between March 1st, 2020 through April 30th, 2020 who received pulmonary CT angiography and had a quantitative D-dimer lab drawn within 24 hours of CT imaging.
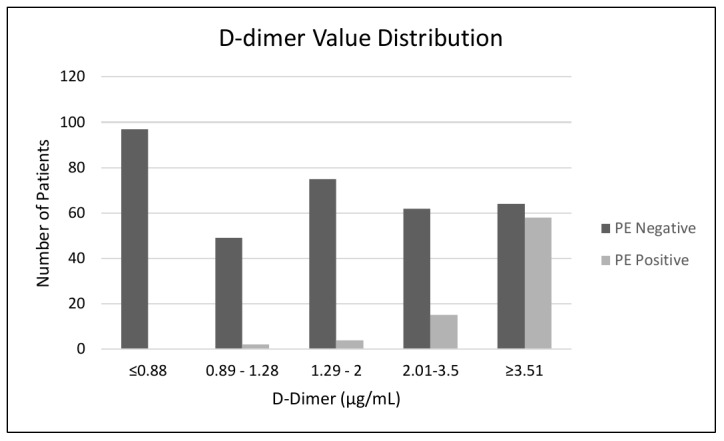
Results: Our sampling criteria yielded a total of n = 426 patients, of whom 347 (81.5%) were negative for PE and 79 (18.5%) were positive for PE. The average D-dimer in the negative PE group was 2.95 μg./mL. (SD 4.26), significantly different than the 9.15 μg./mL. (SD 6.80) positive PE group (P < 0.05; 95% CI -7.8, -4.6). Theoretically, applying the traditional ≤ 0.5 μg./mL. D-dimer cut-off to our data would yield a sensitivity of 100% and specificity of 7.49% for exclusion of PE. Based on these results, the authors would be able to increase the D-dimer threshold to < 0.89 μg./mL. to maintain their sensitivity to 100% and raise the specificity to 27.95%. Observing a D-dimer cut-off value of ≤ 1.28 μg./mL. would reduce sensitivity to 97.47% but increase the specificity to 57.93%.
Conclusions: These study results support the utilization of alternative D-dimer thresholds to exclude PE in COVID-19 patients. Based on these findings, providers may be able to observe increased D-dimer cut-off values to reduce unnecessary pulmonary CT angiography scans.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


